Endotracheal Intubation Preparation, SOAP-ME Mnemonic, CRASH Mnemonic, Physiologic Optimization Prior to Intubation, Prevention of Post-Intubation Hypotension, High Risk Conditions in Airway Management
- See Also
- Advanced Airway
- Rapid Sequence Intubation
- Endotracheal Tube
- Endotracheal Intubation Preoxygenation (and Apneic Oxygenation)
- Direct Laryngoscope
- Video Laryngoscope
- Endotracheal Intubation
- Extraglottic Device (e.g. Laryngeal Mask Airway or LMA)
- Tactile Orotracheal Intubation (Digital Intubation)
- Nasotracheal Intubation
- Cricothyrotomy
- Needle Cricothyrotomy
- Emergency Decision Cycle (OODA Loop, AAADA Model)
- Approach
- Emergency Preintubation Back-up Plan
- See Emergency Decision Cycle (OODA Loop, AAADA Model)
- Review anticipated difficulties in airway management
- Anticipate difficult mask ventilation (MOANS Mnemonic, ROMAN Mnemonic)
- Anticipate difficult Direct Laryngoscopy (LEMON Mnemonic)
- Anticipate difficult Extraglottic Device (RODS Mnemonic)
- Anticipate difficult Cricothyrotomy (SHORT Mnemonic, SMART Mnemonic)
- Levitan describes an emergency back-up parachute approach to intubation
- Every step in intubation should have a back-up plan (Boy Scout "Be Prepared" motto)
- Two ways to ventilate
- Two ways to oxygenate
- Two ways to intubate
- UMMC Shock-Trauma Advanced Airway Plan (Plan A, B, C...)
- Intubation attempt with any technique
- Intubation attempt using Video Laryngoscope and Gum Elastic Bougie
- Intubation attempt by back-up provider (or attending physician)
- Attempt Supraglottic Airway (e.g. Laryngeal Mask Airway)
- Surgical airway (Cricothyrotomy)
- Be prepared for Cricothyrotomy
- Have plan A and plan B (see above)
- Also have a "Go to Hell Plan" in case of "Can't Oxygenate, Can't Intubate"
- Palpate the neck for the cricothyroid membrane prior to each intubation
- Cricothyrotomy kit should be immediately available in case of complete airway obstruction
- Have plan A and plan B (see above)
- Be prepared for failed definitive airway placement
- Have Extraglottic Device (e.g. Laryngeal Mask Airway or LMA) available (with practiced use)
- Have at least two methods of laryngeal exposure immediately available (with practiced use of each)
- Have at least 2 Endotracheal Tubes available
- Estimated size for the patient's body habitus
- One Endotracheal Tube size smaller than expected
- Have two oxygen sources (not on splitter)
- Preoxygenation oxygen source (e.g. Non-Rebreather Mask with reservoir at 12 LPM)
- Apneic Oxygenation source (High Flow Nasal Cannula oxygen source at 15 LPM)
- Have two suction devices
- Open suction tubing without suction tip
- Yankauer suction (or preferably a better tip such as “S3,” “Big Stick,” or “Big Yank” )
- Preparation
- Mnemonic - SOAP-ME
- Suction
- Yankauer suction (or better alternative as above)
- Second suction tubing with no tip attached
- Oxygen
- High Flow Oxygen device (e.g. Non-Rebreather Mask with reservoir)
- Consider CPAP or BIPAP for preoxygenation
- Second oxygen source with Nasal Cannula (up to 15L/min) for Apneic Oxygenation
- Airway equipment
- Patient Positioning
- Pull Mandible forward
- Sit patient up semi-Fowler position (at least 20 degrees) into ramped position of head and trunk (especially if obese)
- Reverse Trendelenburg if patient cannot be flexed at waist (e.g. Hip Fracture)
- Inclined torso improves oxygenation, Lung Volumes and glottis view, and decreases aspiration risk
- Khandelwal (2016) Anesth Analg 122(4): 1101-7 [PubMed]
- Ear to sternal notch
- http://www.emdocs.net/novel-tips-airway-management/
- Head parallel with ceiling
- Ear tragus at level of sternal notch
- Adjust overall bed height to align patient to clinician
- Patient's face should be at xiphoid of clinician for optimal intubation angle
- Monitoring Equipment
- Telemetry
- Oxygen Saturation
- Capnography (End-Tidal CO2)
- Preparation
- Preintubation General Measures
- Prepare for Rapid Sequence Intubation
- Indicated if not crash airway or awake intubation needed for difficult airway
- Monitoring Telemetry, Capnography and Pulse Oximetry (Hypoxemia, Bradycardia)
- Pretreatment with Atropine 0.02 mg/kg is no longer recommended
- Some pediatric providers have it ready at itubation in case of Symptomatic Bradycardia (esp. age under 1 year)
- Check Laryngoscope for light and blade size (See above)
- Video Laryngoscopy is superior to Direct Laryngoscopy for successful first-pass intubation (by Odds Ratio >2)
- Video Laryngoscopy is also associated with reduced risk of esophageal intubation
- However, no difference in poor outcomes when compared with Direct Laryngoscopy
- De Jong (2014) Intensive Care Med 40(5): 629-39 [PubMed]
- Direct Laryngoscope (with working bulb and battery)
- When Video Laryngoscopy fails, Direct Laryngoscopy is the most common rescue device
- Video Laryngoscopy is superior to Direct Laryngoscopy for successful first-pass intubation (by Odds Ratio >2)
- Suction (critical for all patients, especially for children)
- Two suction tubes are ideal (one Yankauer and one with tubing only to suction large particulate matter)
- Select ET size and length (See Endotracheal Tube)
- Cuffed ET Tubes may be used in infants and children
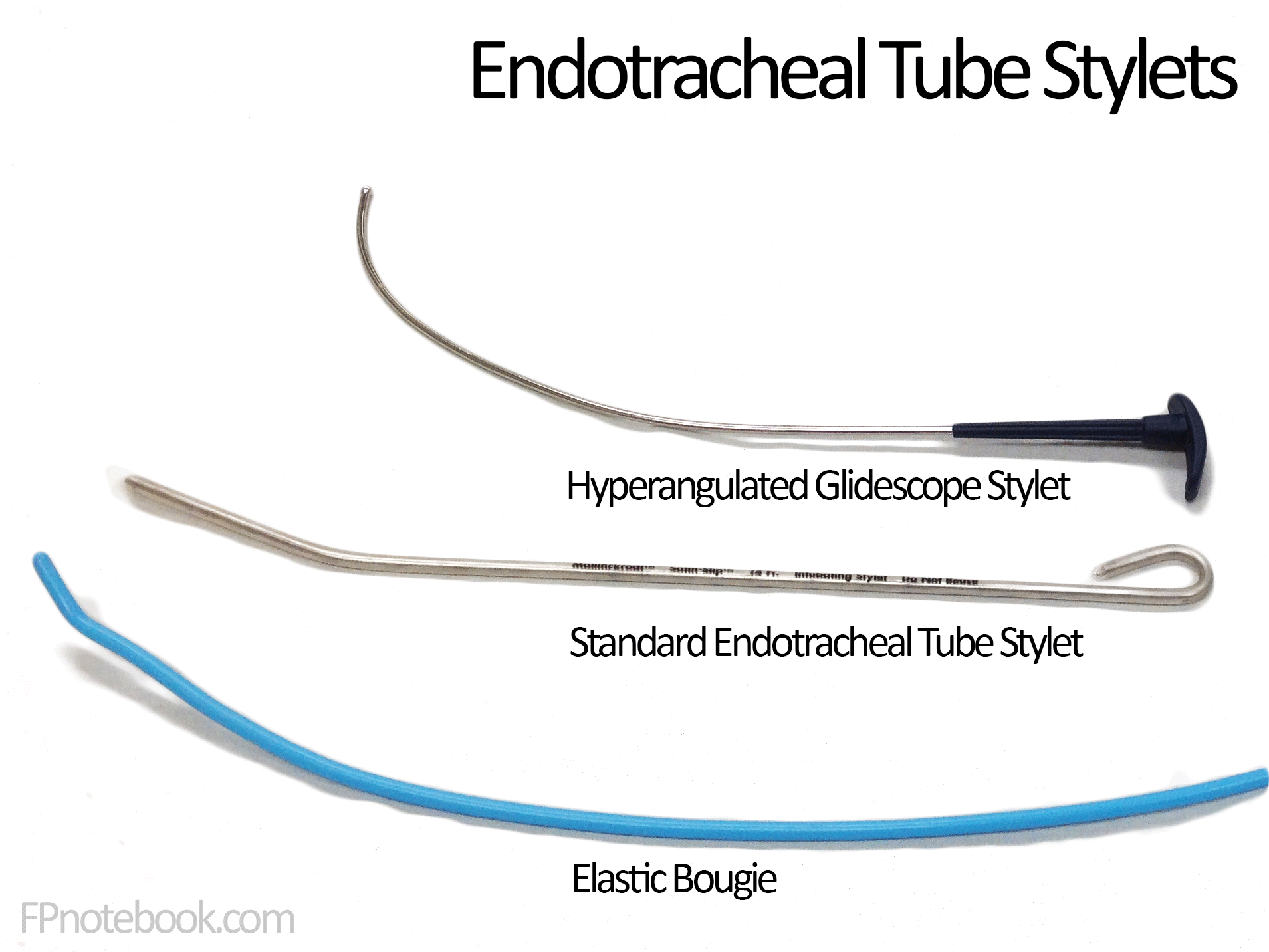
- Endotracheal Tube (including a size smaller than anticipated)
- Stylet should NOT extend beyond distal ET
- Glidescope intubation requires glidescope stylet with deep hockey-stick bend
-
Elastic Bougie
- Curl into a tight loop if using a hyperangulated Laryngoscope Blade (e.g. Glidescope)
- Images
- Approach
- Physiologic Optimization Prior to Intubation (Mnemonic: CRASH)
- Consumption of Oxygen Increased (outpaces Oxygen Delivery)
- Causes: High demand states (e.g. ARDS, Sepsis, pregnancy, children, Thyroid Storm)
- Endotracheal Intubation Preoxygenation (includes Apneic Oxygenation)
-
Right Ventricular Failure
- See Acute Right Ventricular Failure Management
- Right ventricle poorly compensates for increased right-sided Afterload (pulmonary vascular resistance)
- RV has only Tachycardia and a marginal increase in contractility for compensation
- Pulmonary pressures further increase with hypercapnia, Hypoxia, Atelectasis and PPV
- Catastrophic decompensation and Cardiac Arrest may follow
- Acidosis Metabolic
- Hypercapnea during intubation may worsen an already severe Metabolic Acidosis
- Acidosis may precipitate further decreased inotropy and ventricular Arrhythmias
- Saturation of oxygen may fall with prolonged intubation
- Preoxygenation is limited in severe airspace diseases where FRC Is low (e.g. ARDS) or low V/Q (shunt)
- Continue Apneic Oxygenation throughout intubation (e.g. Nasal Cannula at 15 lpm)
- Adequate preoxygenation (tight oxygen mask at 100% FIO2) allows for a safe apneic period during intubation
- Leads to denitrogenation, improved Functional Residual Capacity (FRC), decreased V/Q mismatch
-
Hypotension
- See below
- Optimize underlying conditions before intubation and have Vasopressors readily available
- References
- Brown (2022) Walls Manual of Emergency Airway Management, LWW, p. 21-2
- Approach
- High Risk Conditions in Airway Management
-
Trauma and Hemorrhagic Shock
- See Primary Survey Airway Evaluation
- See Hemorrhagic Shock
- Optimization prior to Endotracheal Intubation
- See physiologic optimization above
- See Endotracheal Intubation Preoxygenation
- Adequate Hemorrhagic Shock Management to prevent Peri-Intubation Hypotension and Cardiac Arrest
- Aggressive Resuscitation before intubation for Hypotension or Shock Index >=0.8
- Use a hemodynamically neutral induction agent (e.g. Etomidate, Ketamine)
- Maintain Cervical Spine Immobilization
- Video Laryngoscopy with hyperangulated blade or bougie assisted intubation may be needed
- Anticipate Trauma distorted Head and Neck Anatomy
- High risk for can oxygenate, can't ventilate scenarios
-
Increased Intracranial Pressure
- Poor neurologic outcomes are associated with Hypoxia, hypercapnia or Hypotension
- Maintain parameters throughout the peri-intubation period
- Maintain Oxygen Saturation >94%
- Maintain PaCO2 35 to 45 mmHg
- Maintain Mean Arterial Pressure (MAP) >80 mmHg
- Other measures
-
Upper Gastrointestinal Bleeding
-
Peri-Intubation Hypotension risk (and Cardiac Arrest risk)
- Adequate Hemorrhagic Shock Management to prevent Peri-Intubation Hypotension and Cardiac Arrest
- Aggressive Resuscitation before intubation for Hypotension or Shock Index >=0.8
- Aspiration risk during intubation
- Raise the head of the bed during intubation
- Blood obscured glottic view
- Have 2 suctions available (e.g. Open suction tubing and Yankauer suction)
- Elevate head of bed
- Consider Nasogastric Tube placement prior to intubation
- Be ready with double set-up for failed airway (e.g. Cricothyrotomy with neck marked)
- Consider using suction tip to lead in front of the Laryngoscope (SALAD technique)
- Examiner holds Laryngoscope in left hand and suction in right
- Suction can also be used to retract the right side of the mouth to improve visibility
- May push suction catheter to the left side and leave in place while passing bougie
- Held together with Laryngoscope in left hand
- If catheter tip large enough, may pass suction tip through cords and bougie through catheter
- Bougie will fit through a large bore suction catheter tip (but not a yanker)
- Consider intubation of the Esophagus and inflating the balloon
- Push esophageal ET Tube to the left side (out of the way, but blocking GI secretions)
- Then intubate the trachea
- References
- Strayer in Herbert (2018) EM:Rap 18(11):1-3
-
Peri-Intubation Hypotension risk (and Cardiac Arrest risk)
-
Cardiac Tamponade
-
Endotracheal Intubation risks Hypotension and Cardiac Arrest in Cardiac Tamponade patients
- Positive Pressure Ventilation increases intrathoracic pressure, decreasing Preload
- Induction agents decrease Cardiac Output and Peripheral Vascular Resistance
- Best to avoid Endotracheal Intubation before Pericardiocentesis (if possible)
- Technique if Endotracheal Intubation is unavoidable
- Optimize Preload with IV fluid boluses of 250 to 500 ml crystalloid
- Consider awake intubation with Ketamine
- Ventilator settings: Low Tidal Volume and low PEEP
-
Endotracheal Intubation risks Hypotension and Cardiac Arrest in Cardiac Tamponade patients
-
Aortic Stenosis
- Prevent Peri-Intubation Hypotension (Cardiac Arrest risk)
- Manage significant Arrhythmias (tachy or brady) prior to intubation
- Have Push Dose Pressors (esp. Phenylephrine for Aortic Stenosis) available at bedside during intubation
- Morbid Obesity
- Head of the Bed at 25 to 30 degrees
- Preoxygenation with noninvasive Positive Pressure Ventilation
- Use two person technique for bag-valve-mask ventilation
- Place blankets or pillows behind the head and neck to align external auditory canal with the sternal notch
- Have a Supraglottic Device (e.g. LMA) available in case of failed airway
- Pregnancy
- See Cardiopulmonary Resuscitation in Pregnancy
- See Trauma in Pregnancy
- High rates of failed Endotracheal Intubation
- Difficult glottic views
- Decreased oxygen reserve
- Increased aspiration risk
- Difficult passage of Endotracheal Tube
- Approach
- Prepare for difficult airway (see above)
- Employ adequate preoxygenation and Apneic Oxygenation
- Head of bed at 20 to 30 degrees decreases aspiration and Hypoxia risk
- Use smaller diameter Endotracheal Tube (7.0 mm)
- References
- Gill and Maldonado (2024) Crit Dec Emerg Med 38(11): 18-9
- Lentz (2020) J Emerg Med 59(4):573-85 +PMID: 32591298 [PubMed]
- Prevention
- Post-Intubation Hypotension
- Anticipate post-intubation Hypotension (related to sedation, Positive Pressure Ventilation, PEEP)
- Monitor Blood Pressure frequently in the period around intubation
- Post-intubation Hypotension is associated with worse outcomes
- Hypotension occurs in up to 25% of emergency intubations (Cardiac Arrest in 3% of intubations)
- Avoid intubating a severely hypotensive patient (outside of crash airway without RSI)
- RSI, NIPPV and Endotracheal Intubation may all significantly lower Blood Pressure further
- Transition from negative pressure ventilation (diaphragm) to intubation decreases Preload
- Peri-Intubation Hypotension is ominous, and may herald imminent Cardiac Arrest
- Temporize airway and breathing management (Nasal Airway, bipap) during stabilization
- Consider awake intubation
- Predict Hypotension following RSI and intubation (consider fluid bolus prior to intubation)
- Extremes of age (children or age >65 years)
- Extremes of body habitus (morbid Obesity or cacchexia)
- Hypoxemia or COPD
- Shock states
- Hypovolemia
- Vasodilatory shock (e.g. Sepsis)
- Cardiogenic Shock
- Shock Index (HR/SBP) > 0.8
- Borderline MAP (65-70 mmHg) pre-intubation
- Even a preintubation SBP <140 mmHg may fall significantly with intubation
- Evaluation
- Consider Arterial Line for Blood Pressure Monitoring
- Place before Radial Pulses are lost
- Arterial Lines remain reliable even in Hypotension and Tachycardia (contrast with Blood Pressure cuffs)
- Consider Inferior Vena Cava Ultrasound for Volume Status
- Fluid responsiveness may be assessed with Passive Leg Raise Maneuver combined with IVC Ultrasound
- IVC <1.5 cm on Ultrasound immediately after intubation, is associated with Hypovolemia
- Consider Arterial Line for Blood Pressure Monitoring
- Management: Optimize systolic Blood Pressure prior to RSI
- Use agents less likely to lower Blood Pressure
- No RSI agents are needed in Cardiac Arrest (crash airway)
- Avoid Propofol as Sedative (induction agent) for emergency intubation
- Choose induction agents with less risk of Hypotension (Etomidate, Ketamine)
- References
- Fluid Resuscitation
- Consider Normal Saline 10-20 ml/kg (to 500 to 1000 ml) bolus prior to RSI (especially in children)
- Standard bolus of crystalloid in a peri-intubation hemodynamically Unstable Patient is 20 cc/kg IV
- Even in CHF, 250 to 500 ml crystalloid bolus is tolerated to stabilize BP for intubation
- Vasopressors
- Optimize mean arterial pressure >80-85 mmHg prior to intubation (fluids, Vasopressors)
- Phenylephrine
- Norepinephrine
- Peri-intubation Norepinephrine is associated with increased mortality in-hospital and 90 day
- Smischney (2015) BMC Res Notes 8:445 [PubMed]
- Other measures
- Consider Delayed Sequence Intubation
- Gradual titration of Ketamine while optimizing oxygenation and mean arterial pressure
- Consider Delayed Sequence Intubation
- Use agents less likely to lower Blood Pressure
- References
- Mallemat in Herbert (2017) EM:Rap 17(2): 4-5
- Weingart and Swaminathan in Herbert (2021) EM:Rap 21(10): 3-5
- Prevention
- Aspiration
- Decompress Bowel Obstruction with Orogastric Tube prior to intubation
- Vomiting otherwise may be profuse and result in significant aspiration and very difficult intubation
- Resources
- Airway Cam (Levitan)
- References
- Levitan (2013) Practical Airway Management Course, Baltimore
- Weingart et al in Herbert (2016) EM:Rap 16(11): 4-5