Arterial Blood Gas, Blood Gas, ABG, PaCO2, PCO2, PaO2, pO2, Arterial Oxygen Partial Pressure
- Labs
- See Venous Blood Gas
- Arterial Blood Gas
- See Arterial Puncture
- See Arterial Line
- Indications
-
Respiratory Failure
- Evaluate alveolar ventilation (PaCO2)
- Evaluate blood oyxgenation (PaO2)
- Evaluate gas exchange (PaO2, PaCO2, A-a Gradient)
- Monitor clinical improvement on NIPPV or Mechanical Ventilation (pH, PaCO2)
- Metabolic Conditions
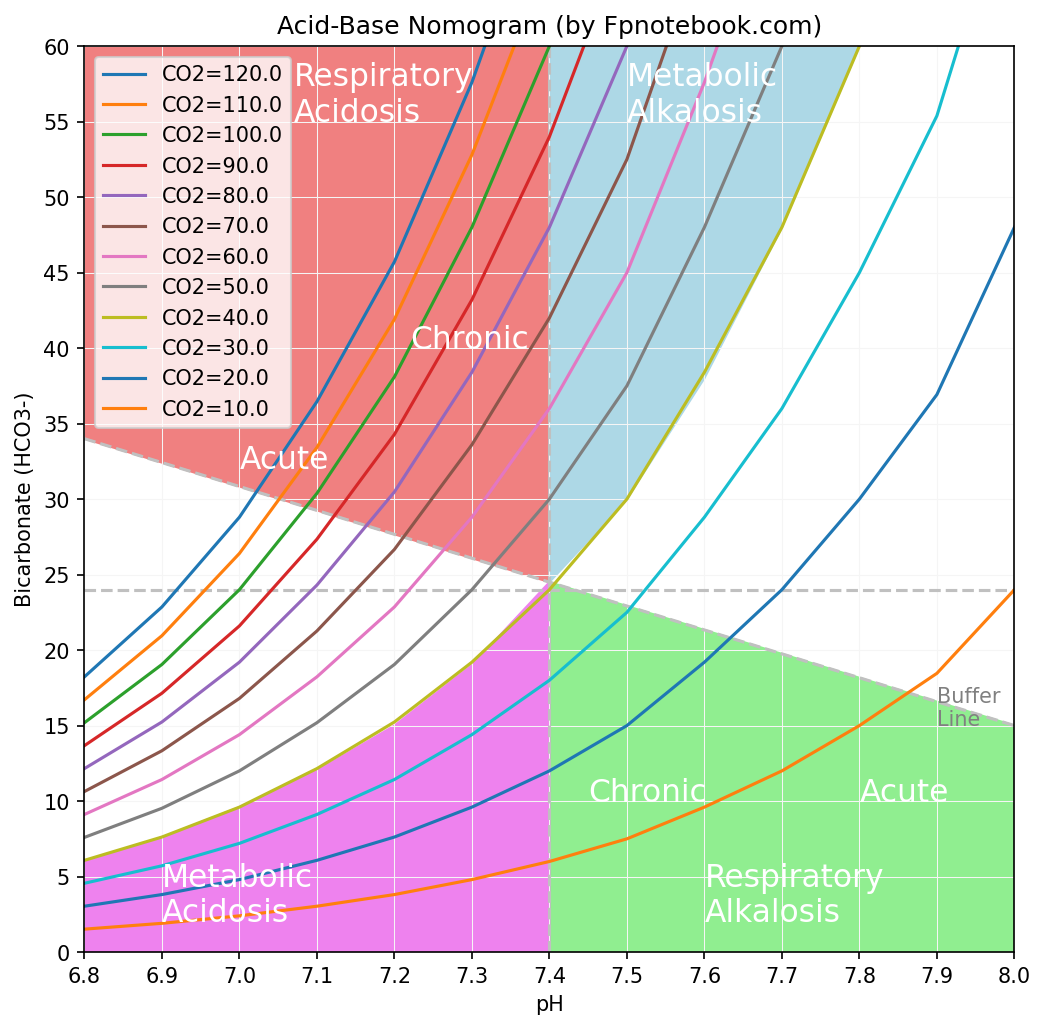
- Images
- AcidBaseNomogram
- Causes
- Primary and Secondary Acid Base Disorders
-
Respiratory Acidosis (pCO2 increases)
- Uncompensated pH decreased = (Normal HCO3)/(Increased pCO2)
- Compensated by Metabolic Alkalosis (HCO3 increases)
- Compensated pH normalizes = (Increased HCO3)/(Increased pCO2)
-
Respiratory Alkalosis (pCO2 decreases)
- Uncompensated pH increased = (Normal HCO3)/(Decreased pCO2)
- Compensated by Metabolic Acidosis (HCO3 decreases)
- Compensated pH normalizes = (Decreased HCO3)/(Decreased pCO2)
-
Metabolic Acidosis (HCO3 decreases)
- Uncompensated pH decreased = (Decreased HCO3)/(Normal pCO2)
- Compensated by Respiratory Alkalosis (PCO2 decreases)
- Compensated pH normalizes = (Decreased HCO3)/(Decreased pCO2)
-
Metabolic Alkalosis (HCO3 increases)
- Uncompensated pH increased = (Increased HCO3)/(Normal pCO2)
- Compensated by Respiratory Acidosis (PCO2 increases)
- Compensated pH normalizes = (Increased HCO3)/(Increased pCO2)
- Mixed Respiratory Acidosis and Metabolic Acidosis (pCO2 increases and HCO3 decreases)
- pH decreased = (Decreased HCO3)/(Increased pCO2)
- Mixed Respiratory Alkalosis and Metabolic Alkalosis (pCO2 decreases and HCO3 increases)
- pH increased = (Increased HCO3)/(Decreased pCO2)
- Interpretation
- pH
- See ABG Interpretation
- See Calculated PaCO2
- Normal arterial pH = 7.36 to 7.44
- ABG and VBG are equivalent in pH accuracy
- VBG pH is consistently 0.03 lower than ABG pH
- Metabolic Conditions are suggested if
- pH changes in the same direction as pCO2
- pH is abnormal but pCO2 remains unchanged
- Metabolic Conditions related changes in Bicarbonate
- Increase pH by 0.01 (with PaCO2 unchanged)
- Bicarbonate increases 0.67 meq/L
- Decrease pH by 0.01 (with paCO2 unchanged)
- Bicarbonate decreases 0.67 meq/L
- Increase pH by 0.01 (with PaCO2 unchanged)
- Interpretation
- PaO2 (Partial Pressure of arterial oxygen)
- See ABG Interpretation
- See A-a Gradient
- See Arterial Blood Oxygen Content (Oxygen Saturation, CaO2)
- Normal PaO2
- Room air at sea level: 80-100 mmHg
- Age Adjusted PaO2 = 100 mmHg – 0.3 * AgeY
- Where AgeY is age in years
- Adjusted for FIO2
- Approximate Normal PaO2 = FIO2 * 5
- Normal PaO2/FiO2 >400 mmHg
- Normal oxygen pressures drop from atmospheric levels to intracellular levels
- Atmospheric oxygen: 160 mmHg
- Alveolar capillary oxygen (PAO2): 105 mmHg
- Arterial oxygen (PaO2): 95 mmHg
- Peripheral interstitial oxygen: 40 mmHg
- Peripheral intracellular oxygen: 25 mmHg
- Peripheral cells need only PO2 of 2 mmHg for adequate functioning
- Venous oxygen: 40 mmHg
-
Hypoxemia
- See Hypoxia
- PaO2 < 50 mmHg
- Interpretation
- PaCO2
- See ABG Interpretation
- See Calculated PaCO2 (Winter's Formula)
- See End Tidal Carbon Dioxide (EtCO2)
- Normal PaCO2: 35-45 mmHg
- Normal carbon dioxide pressures change little throughout circulation (and are much higher than atmospheric levels)
- Atmospheric CO2: 0.3 mmHg
- Alveolar and Arterial CO2: 40 mmHg
- Interstitial, Intracellular and Venous CO2: 45 mmHg
- Respiratory Acidosis with increased PaCO2 consistently affects pH and bicarbonate
- Acute: PaCO2 increase of 10 mmHg increases bicarbonate 1 mEq and decreases pH 0.08
- Chronic: PaCO2 increase of 10 mmHg decreases pH 0.03
- Increased CO2 production is rapidly compensated by increased alveolar ventilation
- An elevated PaCO2 suggests inadequate alveolar ventilation (e.g. Bellows Failure)
- Doubling alveolar ventilation results in half the PaCO2
- Increasing Respiratory Rate from 12 to 24, decreases PaCO2 from 40 to 20 mmHg
- Cutting by half the alveolar ventilation results in double the PaCO2
- Decreasing Respiratory Rate from 12 to 6, increases PaCO2 from 40 to 80 mmHg
- Normal carbon dioxide pressures change little throughout circulation (and are much higher than atmospheric levels)
- Hypercapnia (Hypercarbia, CO2 Retention)
- Interpretation
- Bicarbonate
- See ABG Interpretation
- Normal Bicarbonate (HCO3-): 22-28 mmHg
- Serum bicarbonate is most accurate (compared with ABG or VBG bicarbonate)
- Interpretation
- Conditions Invalidating or Modifying ABG Results
- Delayed analysis
- Iced Sample maintains values for 1-2 hours
- Un-iced sample quickly becomes invalid
- PaCO2 rises 3-10 mmHg/hour
- PaO2 falls at a rate related to initial value
- pH falls modestly
- Excessive Heparin
- Dilutional effect on results
- Decreases bicarbonate and PaCO2
- Large Air bubbles not expelled from sample
- PaO2 rises 0-30 mmHg
- PaCO2 may fall slightly
-
Fever or Hypothermia
- Machine Temperature approaches 37 C
- Patient Temperature shifts oxyhemoglobin curve
-
Hyperventilation or breath holding (due to anxiety)
- May lead to erroneous lab results
- Resources
- Acid-Base Interpreter (fpnotebook)
- ABG Interpretation (unbound medicine)
- ABG Nomogram

- Code for the ABG nomogram is included in Jupyter Notebook

- References
- Arieff (1993) J Crit Illn 8(2): 224-46 [PubMed]
- Narins (1982) Am J Med 72:496 [PubMed]
- Narins (1980) Medicine 59:161-95 [PubMed]
- Ghosh (2000) Fed Pract p. 23-33
- Rutecki (Dec 1997) Consultant, p. 3067-74
- Rutecki (Jan 1998) Consultant, p. 131-42