Cricothyrotomy, Surgical Cricothyrotomy, CriCon, Emergency Tracheostomy Via Cricothyroid Membrane, SHORT Mnemonic, SMART Mnemonic
- See Also
- Advanced Airway
- Rapid Sequence Intubation
- Endotracheal Intubation Preparation
- Endotracheal Tube
- Endotracheal Intubation Preoxygenation (and Apneic Oxygenation)
- Direct Laryngoscope
- Video Laryngoscope
- Endotracheal Intubation
- Extraglottic Device (e.g. Laryngeal Mask Airway or LMA)
- Tactile Orotracheal Intubation (Digital Intubation)
- Nasotracheal Intubation
- Needle Cricothyrotomy
- Background
- Cicothyrotomy is a life-saving definitive tool on the spectrum of airway management interventions
- Indicated in a "Can't Intubate, Can't Oxygenate" (CICO) scenario
- Indicated when other Advanced Airways have been attempted without success
- Cricothyrotomy should not be considered a failure of airway management
- Precautions
- Difficult Cricothyrotomy
- Mnemonic: SHORT
- Surgery (with midline neck scar)
- Hematoma
- Obesity (or other impediments to access, such as C-Collar)
- Radiation Therapy history
- Trauma or Tumor (with distorted Laryngeal Anatomy)
- Mnemonic: SMART
- Surgery (with midline neck scar)
- Mass (Hematoma, abscess or other mass interfering with Cricothyrotomy path)
- Access (C-Collar or brace) or Anatomy (Obesity, redundant tissue)
- Radiation Therapy history to neck
- Tumor (encroaching on the airway)
- Protocol
- Preparation (Cricothyrotomy Tray)
- Tracheal Hook
- Trousseau Dilator
- Scalpel (#11 Blade)
-
Tracheostomy tube (cuffed, unfenestrated, #4)
- Test cuff prior to insertion
- Miscellaneous items
- Gauze 4x4
- Hemostats (small, 2)
- Surgical drape
- Elastic Bougie
- Protocol
- Double-Setup with the CriCon Technique
- Background
- Dr. Scott Weingart on emcrit.org likens Cricothyrotomy preparedness (CriCon) to the old military DefCon system
- Indications
- Assign a Cri-Con level to and prepare for every Advanced Airway placement
- Employ a second airway provider to stand-by at the neck for emergency Cricothyrotomy
- Levels
- Green (Cri-Con 5): All patients undergoing intubation
- Have Cricothyrotomy kit available if needed (check stock)
- Yellow (Cri-Con 4): Anticipated Difficult Airway
- Mark 1.5 cm vertical incision line with skin marker from Thyroid cartilage to cricoid (see below)
- Move Cricothyrotomy kit to bedside
- Red (Cri-Con 3-2-1): Anticipated Failed Airway with no reserve for repeat intubation attempt
- Green (Cri-Con 5): All patients undergoing intubation
- References
- Weingart et al in Herbert (2016) EM:Rap 16(11): 4-5
- EMCrit Blog (Scott Weingart, MD)
- Protocol
- No-Drop Technique
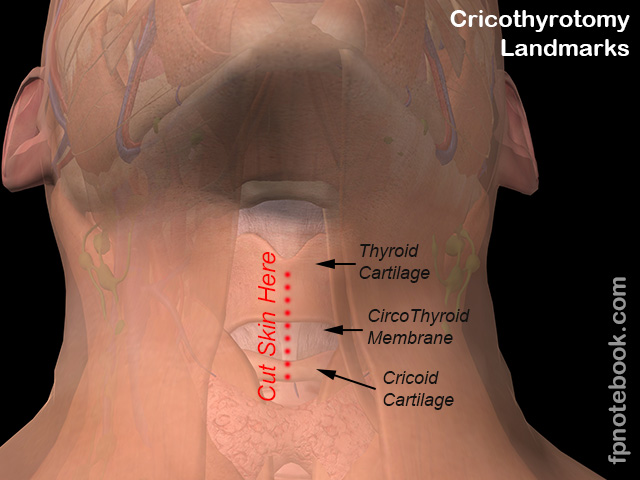
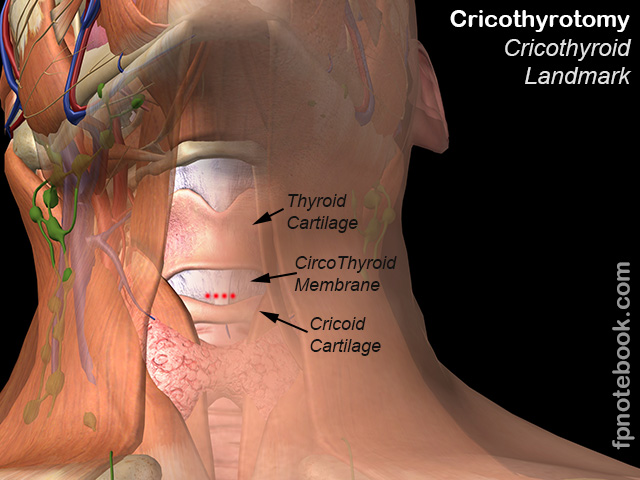
- Identify the landmarks
- Thyroid cartilage
- Cricothyroid membrane
- Cricoid cartilage
- Place fingers at sternal notch
- Slide fingers up, in midline, over the top of each tracheal ring
- Cricoid cartilage will be the first significant bump palpated
- Mark the incision line with skin marker
- Draw vertical line down midline from mid-Thyroid cartilage to cricoid cartilage
- Consider Ultrasound (linear probe) to identify landmarks when soft tissue obscures the cricothyroid membrane and airway

- Prepare the skin
- Antiseptic solution (e.g. Hibiclens, Betadine)
- Lidocaine 1% with Epinephrine infiltrated into skin and subcutaneous tissue down to cricothyroid membrane
- Even in a sedated patient, the Epinephrine may reduce bleeding
- Immobilize the Larynx
- Vertical Skin Incision (superficial)
- Make superficial vertical 2 cm incision
- Incise in midline from mid-Thyroid cartilage to cricoid ring
- Insert index finger to palpate cricothyroid membrane
- Some providers skip the vertical incision if they can easily identify the cricothyroid membrane
- They move straight to making a horizontal incision below
- Reduces bleeding and time to "cut to air"
- However, greater risk of straying off the midline
- Horizontal cricothyroid membrane incision

- Make horizontal incision at lower aspect of membrane (avoids vessels at top of membrane)
- Blood and soft tissue shifting will quickly obscure landmarks (and will spray blood)
- Posterior aspect of cricoid cartilage serves as a long backstop
- Prevents knife from penetrating deep structures
- Technique: Make stab incision through membrane
- Cut to one direction, rotate blade 180 degrees, and cut opposite direction
- Hole must be wide enough to fit a finger, bougie and tube
- Immediately place finger or Elastic Bougie through incision into airway to hold position open
- Option 1: Bougie and 6.0 or 6.5 ET Tube rapid technique (scalpel-finger-tube)
- Immediately move to 6.0 or 6.5 Endotracheal Tube over Elastic Bougie (without inserting hook)
- http://emcrit.org/wee/real-surgical-airway/
- http://emcrit.org/wp-content/uploads/2014/08/EMA-Scalpel-FInger-Bougie.pdf
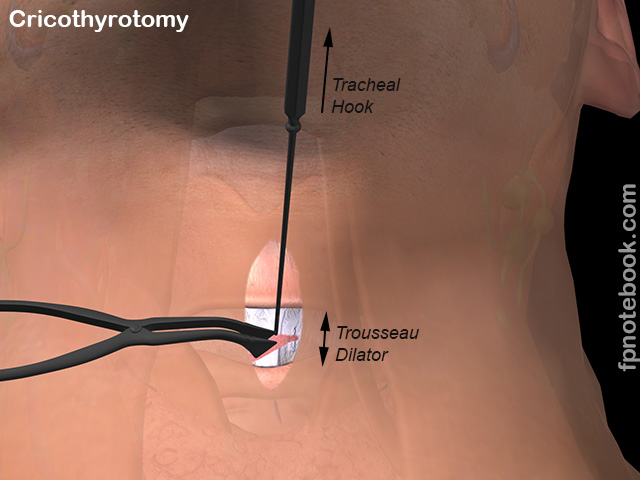
- Option 2: Tracheal hook and dilator
- Insert tracheal hook
- Insert through hook incision
- Rotate hook so it retracts the upper membrane in cephalad direction

- Insert Trousseau dilator
- Dilator is inserted a short distance
- Spread the membrane vertically
- Insert tracheal hook
- Option 1: Bougie and 6.0 or 6.5 ET Tube rapid technique (scalpel-finger-tube)
- Insert Tracheostomy tube
- Consider first inserting Elastic Bougie as guidewire for the Tracheostomy tube (see above)
- Consider 6.0 or 6.5 Endotracheal Tube in place of standard Shiley Tracheostomy tube
- Use an ET Tube that is shortened to 11 cm (alternatively, 6.0 Portex cuffed trach tube may be used)
- ET Tube is inserted only until balloon is completely inside incision, then inflated
- ET Tube is more easily inserted and managed
- Less interlocking parts than Shiley
- Shiley diameters are not consistent and may not allow Gum Elastic Bougie passage
- Insert Tracheostomy tube gently (avoid creating a false passage)
- Rotate so tube is directed towards Bronchi
- Remove dilator and hook (if used)
- Inflate Tracheostomy cuff
- Confirm tube placement
- Auscultate lung fields
- CO2 Detector or Capnography (or consider esophageal detector in Cardiac Arrest)
- Observe for subcutaneous Emphysema
- Suggests paratracheal insertion via false passage
- A Nasogastric Tube or Elastic Bougie inserted into tube will meet significant resistance if tube is mal-placed
- Completion
- Obtain Chest XRay
- Secure tube in place
- Tape (2 inch) split in half at each end and each half wrapped around tube (and other part of tape to chest)
- Respiratory therapy may have more secure ways to fix the tube in position
- Management
- Post-Cricothyrotomy
- Consult pulmonology or Anesthesia for controlled attempt at intubation from above (e.g. under bronchoscopy)
- Consult otolaryngology for further management of Cricothyrotomy site
- Resources
- EM Crit: Surgical Airway (Scott Weingart)
- References
- Brown (2022) Walls Manual of Emergency Airway Management, LWW
- Levitan (2013) Practical Airway Management Course, Baltimore
- Majoewsky (2012) EM:Rap-C3 2(9): 6
- Walls (2008) Emergency Airway Management, Lippincott, Philadelphia, p. 193-220