Sodium and Water Homeostasis, Fluid Homeostasis, Sodium Hemeostasis, Fluid Shifts, Osmoregulation, Water-Electrolyte Balance, Sodium, Sodium Cation, Fluid and Electrolyte Balance
- See Also
- Physiology
- Total blody water distribution
- See Total Body Water
- Images
-
Total Body Water (TBW) accounts for 60% of body weight in men (50% in women)
- Example: 70 kg man has ~42 L TBW and a 70 kg woman has ~35 L TBW
- Free water flow between ECF and ICF compartments follows the chief solutes for each compartment
- Sodium (Na+) is the primary extracellular fluid solute
- Potassium (K+) is the primary intracellular fluid solute
- Edelman equation summarizes the relationship between water and key solute concentrations
- Na_conc = (Na_ecf + K_icf)/TBW
- Where
- Na_conc is the total body Sodium concentration
- Na_ecf is exchangeable Sodium from the extracellular fluid (ECF)
- K_icf is exchangeable Potassium from the intracellular fluid (ICF)
- TBW is Total Body Water
- Intracellular fluid volume or ICFV (66% of Total Body Water)
- Extracellular fluid volume or ECFV (33% of Total Body Water)
- Example: 70 kg man has ~14 L ECFV and a 70 kg woman has ~12 L ECFV
- Electrolytes
- Interstitial volume (75% of extracellular fluid)
- Plasma volume (25% of extracellular fluid)
- Plasma is 92% water
- Remainder mostly Protein (albumin, Coagulation Factors, Fibrinolytic Proteins, Immunoglobulins)
- Plasma volume is maintained by plasma Proteins via oncotic pressure
- Plasma volume represents 55% of Blood Volume (3L in a 70 kg male)
- Remaining 45% of Blood Volume is cellular (Red Blood Cells, White Blood Cells, Platelets)
- Total Blood Volume from Ideal Body Weight (kg)
- Adult: 7% (5L in 70 kg male)
- Child: 8-9% (80 ml/kg)
- Plasma is 92% water

- Physiology
- Sodium and Water
-
Total Body Water is primarily maintained via extracellular Sodium concentration
- Extracellular Sodium is maintained at 135-145 mEq/L
- Sodium (Na+) is the primary osmole to maintain extracellular fluid volume
- Total body Sodium is typically estimated based only on extracellular Sodium
- Intracellular Sodium is negligible (<20 mEq/L) compared with extracellular Sodium (>135 mEq/L)
- Water follows higher Sodium concentrations (osmotic pressure gradient)
- Increased Sodium concentrations results in greater extracellular water retention
- Results in Fluid Overload (Edematous State) with increased ECFV
- Decreased Sodium concentration results in extracellular water loss
- Results in volume depletion with decreased ECFV
- Increased Sodium concentrations results in greater extracellular water retention
- Sodium is regulated to maintain appropriate extracellular fluid volume
- Sodium homeostasis balances Sodium intake with Sodium excretion
- Fluid Overload and Hypovolemia are defects in Sodium regulation (even when Serum Sodium is normal)
- Hyponatremia is a water excess state (water regulation abnormality)
- May be associated with low, normal or high ECFV (or total body Sodium)
- Physiology
- Osmolality and Tonicity
- See Serum Osmolality (and Extracellular Fluid Tonicity)
- Sodium is the chief osmole in maintaining plasma osmolality and tonicity
-
Osmolal Gap
- Osmolality may be calculated based on known solutes (Sodium, Glucose, BUN)
- Osmolar Gap is the difference between expected and measured osmolality
-
Osmolar Gap >10 mOsm/L suggests unmeasured solutes
- Example: Toxic Alcohols such as Polyethylene Glycol
- Cellular hydration and tonicity
- Fluid Shifts into or out of cells are based on tonicity
- Rapid changes in extracellular Sodium concentration can seriously impact cell fluid (esp. brain cells)
- Rapid onset Hyponatremia, results in cell swelling
- Rapid onset Hypernatremia, results in cell shrinkage
- Physiology
- Sodium Regulation Mechanisms (Renally Mediated)
- Images
- Nephron (Glomerulus and Renal Tubules)
- Sodium freely crosses the glomerular basement membrane
- Of filtered Sodium and water (180 L/day in a healthy 70 kg person), 65% is reabsorbed
- Sodium filtered through glomerulus into renal tubule has same initial concentration as blood
- Water follows Sodium through glomerulus
- Renal Sodium excretion is responsible for most Sodium loss
- Other causes of Sodium loss include sweating, Diarrhea, Hemorrhage and Burn Injury
- Glomerular Filtration Rate (GFR)
- Glomerular-Tubular Balance
- GFR is correlated with Sodium reabsorption in proximal tubule
- Decreased GFR results in decreased filtered Sodium and decreased Sodium and water reabsorption
- Increased GFR results in increased filtered Sodium and increased Sodium and water reabsorption
- Tubulo-Glomerular Feedback
- Glomerular Filtration Rate (GFR) is modulated by the Macula densa in the renal tubule
- Increased tubular flow at Macula densa results in afferent arteriole constriction and decreased GFR
- Decreased tubular flow at Macula densa results in afferent arteriole dilation and increased GFR
- Glomerular-Tubular Balance
- Renal Tubules
- Water reabsorption (without Sodium) is in the descending loop of henle
- Sodium reabsorption (without water) is in the ascending loop of henle
- Results in hyperosmolar interstitium in the lower aspect of the loop of henle region
- Collecting Duct
- Collecting duct passes through the hyperosmolar interstitium and allows for further water reabsorption
- Collecting duct is porous, and water follows osmotic gradient into interstitium, concentrating the urine
- Antidiuretic Hormone (ADH) increases the collecting duct permeability to water (and water reabsorption)
- Sodium freely crosses the glomerular basement membrane
-
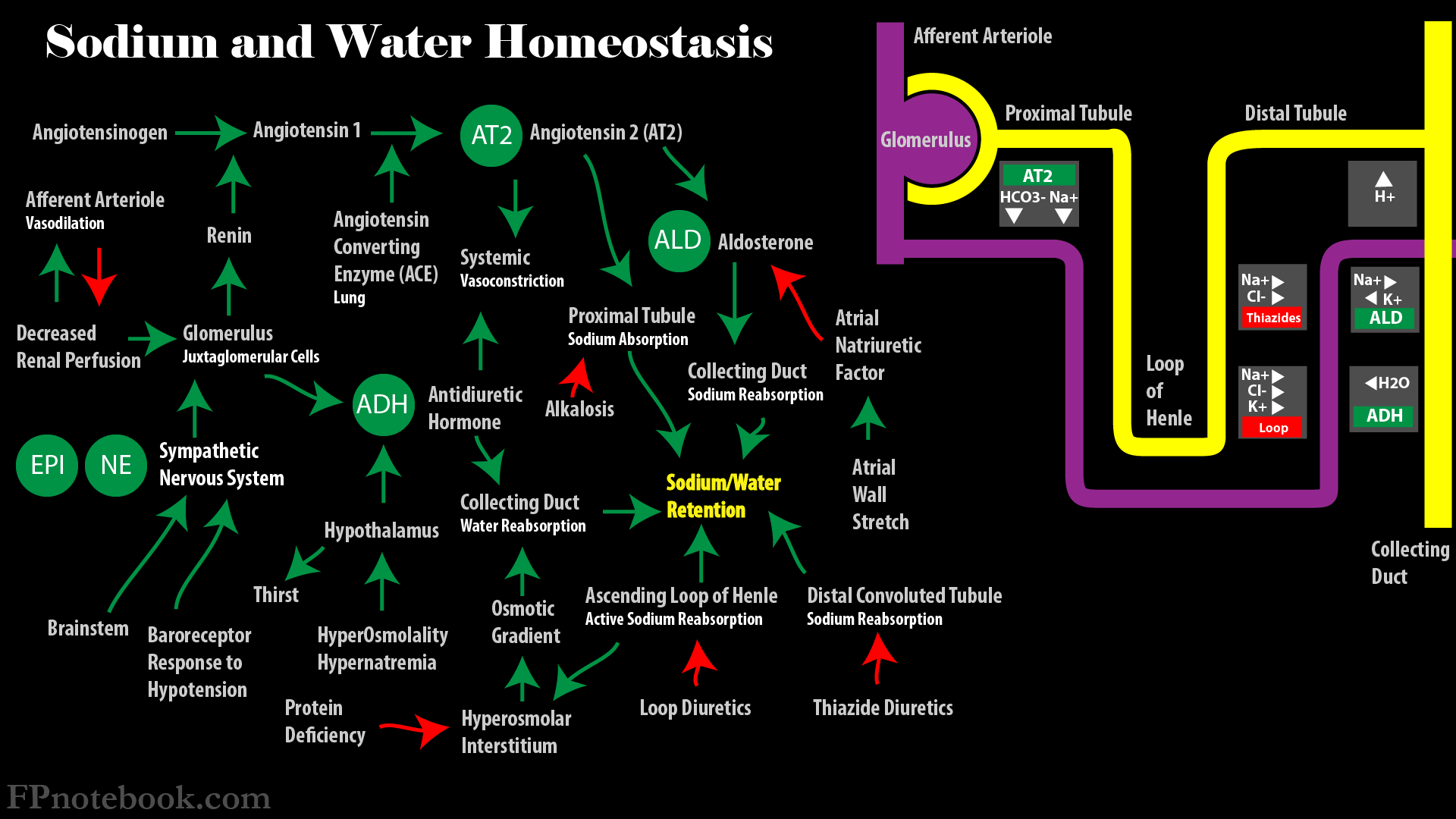
Renin-Angiotensin System (and Aldosterone)
- See Renin-Angiotensin System
- Afferent (sensory)
- Renal juxtaglomerular cells sense decreased renal perfusion and release renin
- Renin converts Angiotensinogen to Angiotensin I
- Angiotensin Converting Enzyme converts Angiotensin I to Angiotensin II
- Efferent (action)
- Angiotensin II stimulates Aldosterone release from the Adrenal Cortex (zona glomerulosa)
- Aldosterone acts to increase Sodium absorption at the distal nephron (cortical collecting tubule)
- Angiotensin II increases proximal tubule Sodium absorption
- Sodium reabsorption is contingent on normal or acidic proximal tubule pH
- Sodium crosses from renal tubule cell into capillary with bicarbonate
- Bicarbonate crosses from renal tubule into renal tubule cell as CO2 via H+
- In alkalosis, H+ is lacking, bicarbonate (and Sodium) is less reabsorbed
- Sodium reabsorption is contingent on normal or acidic proximal tubule pH
- Angiotensin II stimulates Aldosterone release from the Adrenal Cortex (zona glomerulosa)
- Atrial natriuretic factor
- See Brain Natriuretic Peptide (BNP)
- Afferent (sensory)
- Atria and vena cava respond to increased intravascular volume, filling and stretch
- Release atrial natriuretic factor from atria in response to increased volume
- Efferent (action)
- Overall effect is to increase Sodium (and water) excretion by blocking Sodium reabsorption
- Atrial natriuretic factor increases Glomerular Filtration Rate (GFR)
- Dilates afferent glomerular arteriole
- Constricts efferent glomerular arteriole
- Atrial natriuretic factor opposes Renin-Angiotensin System
- Decreases renal Sodium absorption at distal nephron (opposes Aldosterone)
- Inhibits renin secretion
-
Sympathetic Nervous System
- Afferent (sensory)
- Aorta and carotid sinus receptors respond to decreased pressure (low volume)
- Activates Sympathetic System in response to volume depletion (decreased ECFV)
- Efferent (action)
- See Sympathetic Nervous System for effects
- Sympathetic System activation results in renal Sodium retention
- Mediated via Renin-Angiotensin System
- Afferent (sensory)
- Physiology
- General Water Regulation Mechanisms (affects osmolality and tonicity)
- Background
- Water intake and output mechanisms have greatest ECF Sodium concentration effect
- Thirst
- Potent Sensation that increases water intake and prevents Hypernatremia
- Hypernatremia is rare with intact thirst mechanism and adequate water access
- Inducers of thirst
- Increased extracellular fluid osmolality (responds to even a few mOsm/L difference)
- Angiotensin II
- Extracellular Fluid Volume depletion
- Potent Sensation that increases water intake and prevents Hypernatremia
-
Antidiuretic Hormone (ADH or Arginine Vasopressin)
- Overall effect is to increase renal water reaborption
- ADH is released from the posterior pituitary
- Released in response to osmoreceptors in the hypothothalamus detecting hypertonicity
- Hypertonicity also stimulates thirst Sensation
- Response to increased plasma osmolality (and increased plasma Sodium concentration, Hypernatremia)
- Increased ADH secretion
- Water retention by the Kidneys
- Decreased plasma Sodium concentration (and decreased plasma osmolality)
- Response to decreased plasma osmolality (and decreased plasma Sodium concentration, Hyponatremia)
- Decreased ADH secretion
- Free water diuresis
- Increased plasma Sodium concentration (and increased plasma osmolality)
- Abnormal Antidiuretic Hormone
- Syndrome Inappropriate ADH Secretion (SIADH)
- Inappropriate ADH release, resulting in water retention despite normal Sodium and water status
- Results in Isovolemic Hypoosmolar Hyponatremia
- Diabetes Insipidus
- Excessive constant water diuresis due lack of pituitary ADH release or lack of renal response
- Syndrome Inappropriate ADH Secretion (SIADH)
- Renal responses
- See Below
- Hypertonic response (e.g. Hypernatremia)
- Kidney retains water
- Urine is more concentrated than plasma
- Hypotonic response (e.g. Hyponatremia)
- Kidney excretes water
- Urine is more dilute than plasma
- Physiology
- Renal Water Regulation Dependencies
- Adequate Glomerular Filtration Rate
- Concentrating and diluting mechanisms require a minimum GFR of 20% of normal
- Adequate renal tubule concentrating and diluting functions
- Adequate glomerular filtrate delivery to tubules
- Excessive proximal tubule water reabsorption bypasses the distal tubule
- Excessive proximal tubule water reabsorption may result in Hyponatremia
- Volume depletion (e.g. free water replacement of Diarrhea losses)
- Edematous States (e.g. CHF, Cirrhosis, Nephrosis)
- Adequate urine concentrating function (Ascending Loop of Henle)
- Ascending loop of henle reabsorbs 30% of Sodium into the Medullary interstitium
- Sodium (but not water) is reabsorbed via the Sodium-Potassium-2-chloride pump
- Sodium reabsorption in ascending loop of henle is blocked by loop diurectics
- However, Sodium may still be reabsorbed in distal convoluted tubule
- Therefore, Loop Diuretics cause less Hyponatremia and greater water loss
- Contrast with Thiazide Diuretics which block distal convoluted tubule
- Hypertonic Interstitium (via active Sodium reabsorption) allows for a concentrated urine
- Hypertonic Medullary interstitium attracts water from the collecting tubule
- Collecting tubule water permeability is increased by ADH (greater water reabsorption)
- Mediators decreasing interstitial hypertonicity and osmotic gradient (less water reabsorption)
- Decreased hypertonicity with Loop Diuretics
- Decreased hypertonicity with Protein deficiency (nutritional deficiency)
- Urea (Protein breakdown) also increases hyperosmolar interstitium
- Adequate urine diluting function (Distal Convoluted Tubule)
- Additional 5-10% of Sodium and chloride are reabsorbed at the distal convoluted tubule
- Sodium chloride reabsorption is blocked by Thiazide diurectics at the distal convoluted tubule
- Thiazide diurectics cause a relative retention of water more than Sodium
- Results in a greater risk of Hyponatremia than with Loop Diuretics
- Without later water reabsorption, the urine is dilute
- Adequate glomerular filtrate delivery to tubules
- Adequate Antidiuretic Hormone (ADH) functioning
- ADH is key regulator of urine concentration and dilution (1200 mOsm/L to 50 mOsm/L)
- Appropriate central ADH release
- ADH is released in response to small increases in extracellular Sodium concentration
- Also released with volume depletion
- Inappropriately increased ADH release with SIADH
- Results in Isovolemic Hypoosmolar Hyponatremia
- Deficient ADH release occurs with Central Diabetes Insipidus
- Results in decreased collecting tubule permeability, water loss and Hypernatremia
- ADH is released in response to small increases in extracellular Sodium concentration
- Appropriate renal ADH response
- ADH increases Medullary collecting tubule water permeability
- Water flows from the collecting tubule into the hypertonic Medullary interstitium
- Inappropriately increased ADH responsiveness with ADH-like drugs
- Results in SIADH
- Deficient ADH response occurs in Nephrogenic Diabetes Insipidus
- Results in decreased collecting tubule permeability, water loss and Hypernatremia
- ADH increases Medullary collecting tubule water permeability
- Physiology
- Images
- Nephron

- References
- Marino (2014) ICU Book, p. 653-72
- Preston (2011) Acid-Base Fluids and Electrolytes, p. 3-30
- Rose (1989) Clinical Physiology of Acid-Base and Electrolyte Disorders, p. 3-27