Burn Injury, Burn Evaluation, First Degree Burn, Second Degree Burn, Burn of Second Degree, Third Degree Burn, Burn of Third Degree, Rule of 9, Rule of Nines, Burn Prevention, Fire-Related Injury, Thermal Burn, Thermal Injury
- See Also
- Epidemiology
- Causes
- High Temperature Liquids or Scald Burn (80% of burns in young children)
- Hot liquids pulled off the counter
- Flame-related burns (more common in school age children and teens)
- Lighters
- Lighter fluid
- Fireworks
- Gasoline
- Contact Burns
- Contact with high Temperature objects
- Pathophysiology
- Thermal Burn injury
- External heat disrupts tissue layers resulting in damage
- Longer heat exposure results in deeper burn injuries
- Deep dermal injury
- Disrupts elasticity, mechanical barrier protection and vascular supply
- Results in scarring and Non-Healing Wounds
- Burn severity is dependent on multiple factors
- Patient specific (e.g. thinner skin at the extremes of age)
- Burn heat source
- Contact time with heat source
- Anatomic burn location (e.g. thicker skin on palms and soles)
- Precautions
- Consider physical abuse
- Intimate Partner Violence
- Elder Abuse
- Nonaccidental Trauma in children with Burn Injury
- Physical abuse accounts for 5-6% of Burn Injury <12 years old
- Social workers typically review pediatric burns at burn centers and pediatric hospitals
- Involve child protective services and pediatric specialty center evaluation if suspected abuse
- Consider in delayed presentation, parental indifference and inconsistent history
- Consider in burns to hands or feet, buttocks or posterior legs
- Consider in well demarcated burns or linear or patterned burns
- Consider in symmetric burns and in those that do not spare the flexor crease
- Flash or flame burns have additional risks (when compared with contact burns)
- Timing after Burn Injury affects presentation
- Early presentations of severe burns may lack Blistering
- Evaluate for other Traumatic Injury (esp. major mechanism, e.g MVA)
-
Altered Mental Status
- Burn Injury alone is typically associated with alert, Agitated Patient in pain
- Decreased level of conciousness (or Seizures) suggests other cause
- Carbon Monoxide Poisoning
- May be associated with Headache, Nausea, Vomiting, Dizziness, myalgias
- Obtain Carboxyhemoglobin level
- Cyanide Poisoning
- Associated with severe acidosis
- May be associated with Syncope or cardiovascular collapse
- Head Trauma
- Carbon Monoxide Poisoning
- Types
- Electrical Injury
- Lightning Injury
- Chemical Toxin
- Fire-Related Injury
- Thermal Burn
- Contact with hot surface and scald burns from liquid (>111 F, 43 C) account for 85% of pediatric burns
- Smoke Inhalation
- Occurs in 5-35% of hospitalized Burn Injury patients
- Acute airway compromise (airway edema)
- Carbon Monoxide Poisoning
- Cyanide Poisoning
- Thermal Burn
- History
- See Trauma History (e.g. SAMPLE History)
- Comorbidities affecting burn healing and complications
- Diabetes Mellitus
- Tobacco Abuse
- Clotting or Bleeding Disorders
- Corticosteroid use
- Comorbidities affecting fluid Resuscitation and Electrolytes
- Congestive Heart Failure
- End-stage renal disease
- Hepatic failure
- Signs
- Burn Degree
- Precaution
- Conversion to deeper burn may occur over ensuing days after initial injury
- First degree (Superficial burn)
- Second degree (Partial thickness burn)
- Superficial partial thickness
- Pathophysiology
- Findings
- Wet, weaping lesions with clear Blisters
- Erythematous, soft skin that blanches with pressure
- When touched, skin is hypersensitive and painful
- Course
- Healing occurs within 14-21 days
- Scarring is possible but uncommon (deeper structures including stem cells are spared)
- Deep partial thickness
- Pathophysiology
- Findings
- Drier lesions than with superficial partial thickness
- White or pale to Yellow Skin that when touched does not blanch (or has decreased blanching)
- Hemorrhagic Blisters may be present
- Painful despite reduced Sensation to touch
- Skin is slightly tense (less soft than in superficial partial thickness burns)
- Course
- Healing typically takes >21 days (3-5 weeks)
- Scarring and contractures are common complications (involves stem cells, follicles, glands)
- Benefits from early evaluation by burn surgeon early operative management
- Superficial partial thickness
- Third degree (Full thickness)
- Pathophysiology
- Kills all skin layers (involves all of Dermis)
- Also involves underlying subcutaneous fat and connective tissue
- Findings
- Waxy, dark-brown to black, tan or white skin
- Skin is stiff and leatherlike (contrast with soft skin of superficial burns)
- Bright red burns without blanching or Sensation are Third Degree Burns (contrast with pink Second Degree Burns)
- No Sensation to touch
- No Capillary Refill
- Course
- Burn center evaluation indicated in all cases
- Typically do not heal without skin grafting
- Contractures are a common complication
- Pathophysiology
- Fourth degree
- Destroys all skin layers
- Also involves Muscle, tendon or bone
- Signs
- Estimating Surface Area with Rule of 9's
- Precautions
- Estimate burn area only based on second and Third Degree Burns
- First Degree Burns do not count for calculation (Sunburn-like red, closed injury areas)
- Exercise caution in burn area calculation in children (overestimated by >200%)
- Can substantially affect fluid Resuscitation volume calculation (Parkland Formula)
- Goverman (2015) J Burn Care Res 36(5): 574-9 +PMID:25407387 [PubMed]
- Lund and Bowder Chart offers a more accurate assessment of burn area
- Estimate burn area only based on second and Third Degree Burns
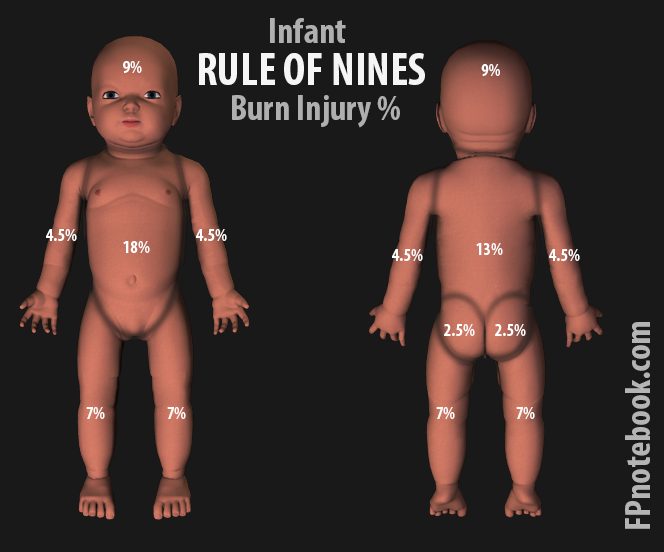
- Infant Rule of 9s

- Head: 18%
- Torso Back: 18%
- Torso Front: 18%
- Leg Left: 14%
- Leg Right: 14%
- Arm Left: 9%
- Arm Right: 9%
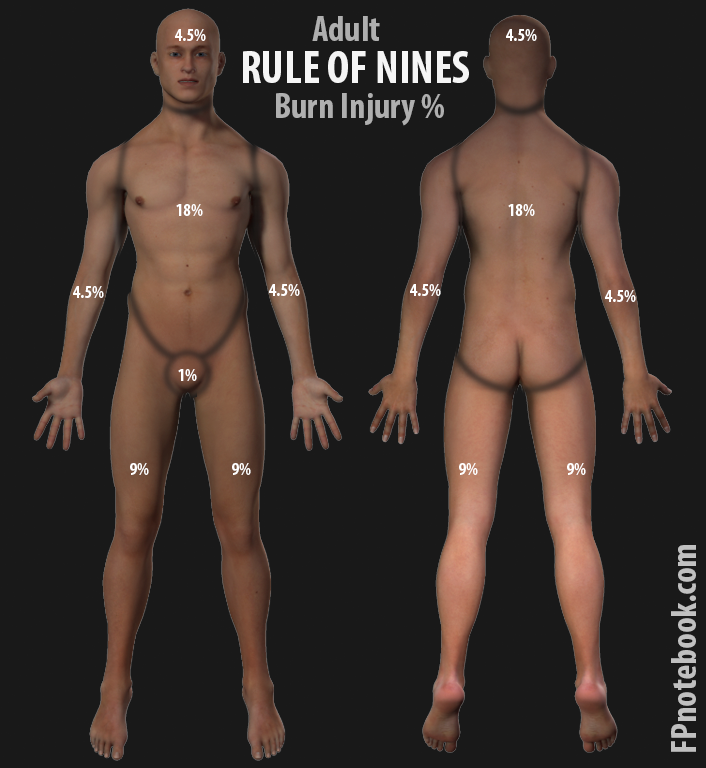
- Adult Rule of 9s

- Torso Front: 18%
- Torso Back: 18%
- Leg Left: 18%
- Leg Right: 18%
- Head: 9%
- Arm Left: 9%
- Arm Right: 9%
- Genitalia: 1%
- Size of patients palm
- Entire palm and fingers: 1% TBSA (inaccurate in obese patients)
- Palm only: 0.5% TBSA
- Resources
- EasyTBSA
- Iphone/Android App - Calculate Body surface area in Burn Injury
- https://apps.apple.com/us/app/easytbsa/id1554943740
- https://play.google.com/store/apps/details?id=org.cnmc.EasyTBSA&hl=en_US&gl=US
- EasyTBSA
- Labs
- Not indicated in minor superficial Burn Injury
- Complete Blood Count
- Comprehensive metabolic panel
- Coagulation studies (PTT, INR)
- Creatinine Kinase (CK)
-
Urinalysis
- Urine Dipstick Blood positive without Red Blood Cells on microscopy may indicate Myoglobinuria
- Electrocardiogram (EKG)
-
Carbon Monoxide Level
- False Negatives may occur at presentation due to prehospital oxygenation
-
Lactic Acid
- May be elevated in cyanide Poisoning (from combustion of synthetic materials in structure fires)
- Venous Blood Gas (VBG) or Arterial Blood Gas (ABG)
- Evaluation
- Minor burn criteria
- Burn is not circumferential
- Burn is only injury
- Burn does not involve high risk areas
- Across major joints
- Face
- Hands or feet
- Perineum or genitalia
- Partial thickness burn surface area is limited (Second Degree Burn area)
- Ages 10 to 50 years old: Burn area <10%
- Age under 10 or over age 50 years old: Burn area <5% (<2% third degree, full thickness)
- Management
- See Burn Management
- Prevention
- Burns in Children
- Consider Nonaccidental Trauma, Intimate Partner Violence or Elder Abuse (see precautions as above)
- Bath
- Test bathwater before placing child in bath
- Set hot water heater to lowest setting (below 120 degrees F)
- Monitor children continuously when in the bath or near faucets
- Kitchen
- Preferentially use the back Burners of the stove when cooking in the presence of children
- Household
- Test smoke alarms on a regular basis
- Monitor children when near fireplace
- Keep children away from matches, fireworks, gasoline and explosives
- Keep children away from hot objects
- Never hold children while working with hot objects
- Prognosis
- Increased mortality risk factors
- Age >60 years
- Associated Smoke Inhalation
- References
- Lindquist and Myers (2025) Crit Dec Emerg Med 39(10): 4-14
- Mason and Yowler in Herbert (2016) EM:Rap 16(4):4-5
- Weir (2020) Crit Dec Emerg Med 34(12): 3-11
- Nemri and Fairbrother (2021) Crit Dec Emerg Med 35(9): 3-10
- Cuttle (2009) Burns 35(6): 768-75 [PubMed]
- Grunwald (2008) Plast Reconstr Surg 121(5): 311e-9e [PubMed]
- Hettiaratchy (2004) BMJ 328(7452): 1366-8 [PubMed]
- Lanham (2020) Am Fam Physician 101(8): 463-70 [PubMed]
- Lloyd (2012) Am Fam Physician 85(1): 25-32 [PubMed]
- Roberts (2003) Emerg Med News 25(3): 28-31 [PubMed]
- Sheridan (2005) Emerg Care 21(7): 449-56 [PubMed]