Wilderness Medicine, Wilderness Trauma, Wilderness Evacuation, Improvised Litter Evacuation
- See Also
- Causes
- Common Wilderness Injury and Illness
- Athletic injuries (sprains, strains and soft tissue Contusions)
- Gastrointestinal symptoms (Nausea, Vomiting, Diarrhea)
- Skin Injuries (Lacerations, Puncture Wounds, Blisters, Burn Injury, Contact Dermatitis)
- Exacerbations of chronic medical conditions (e.g. Asthma, Diabetes Mellitus)
- Upper Respiratory Infections or Influenza-like illness
- Serious Wilderness Trauma and serious illness are uncommon
- Ankle Fractures are the most common Fracture
- Severe Dehydration is uncommon
- Environmental injury (Frostbite, Hypothermia, Heat Illness, altitude sickness) are surprisingly uncommon
- Management
- Trauma
- Constantly reevaluate the safety of both the patient and the provider
- Wilderness first response
- Follow Trauma Primary Survey as able
- Control external Hemorrhage
- Keep patient warm (except where risk of Heat Illness)
- Arrange early evacuation
- Do no harm!
-
ATLS protocol (once in safe, stable environment)
- Primary Survey
- Modified for environment and available equipment (e.g. may not be able to expose patient)
- Resuscitation
- Secondary Survey (including AMPLE History and spine clearance)
- Definitive Plan
- Packaging (including Splinting) and other preparation for transfer
- Primary Survey
- Spine Clearance (all criteria must be met)
- Patient is awake, alert, reliable, not intoxicated and has a normal GCS without neurologic deficit
- Patient is NOT severely injured (i.e. multisystem Trauma) and has no distracting injury (thoracic, proximal long bone)
- Patient does NOT have significant spine pain or tenderness (>=7/10)
- Patient can actively, fully flex, extend and rotate regardless of pain (45 degrees cervical, 30 degrees thoracolumbar)
-
Chest Needle Decompression Indications (Tension Pneumothorax)
- Significant Shortness of Breath
- Hypoxia or Cyanosis
- Distended neck veins
- Tracheal deviation
- Altered Mental Status
- Musculoskeletal Injuries
- See Improvised Splinting Techniques
- Assess CMS (circulation, motor, sensory), joint above, joint below, skin (tenting, puncture) and compartments
- Perform dislocation reductions on scene if safe (and no Fracture is suspected)
- Prolonged long bone Fracture traction (e.g. Femur Fracture) is no longer recommended (risks, lack of benefit)
-
Hemorrhage Management
- See Tourniquet
- U.S. military MARCH protocol emphasizes early control of Hemorrhage (before ABCs)
- Tourniquet application has resulted in dramatic mortality benefit (96% vs 4% survival)
- Kragh (2011) J Emerg Med 41(6): 590-7 [PubMed]
- Management
- Evacuation
- Indications
- Deterioration or lack of improvement after management
- Debilitating pain
- Travel cannot be sustained at a reasonable pace due to a medical condition (may travel toward definitive care)
- Persistent Abdominal Pain (may travel toward definitive care)
- Signs and symptoms of serious high-altitude illness
- Infections that fail to improve after 24 hours of treatment
- Chest Pain not clearly due to minor Musculoskeletal Injury
- Acute psychiatric condition that puts the patient or group at risk (may travel toward definitive care)
- Large wounds or serious injuries with complications
- Open Fracture
- Deformed Fracture
- Impaired neurovascular status
- Gunshot Wound
- Suspected spine injury
- Precautions
- Evacuation is time and labor intensive (anticipate <1 mile/hour)
- Severely ill patients or those with high risk injury may need in-place evacuation (e.g. SAR helicopter)
- Carefully plan evacuation routes that take into account terrain and potential adverse weather conditions
- Evacuation Methods
- Patient hikes out carrying their own gear
- Patient hikes out while others carry their gear
- Litter evacuation by group (with improvised litter)
- Litter evacuation by professional rescue services
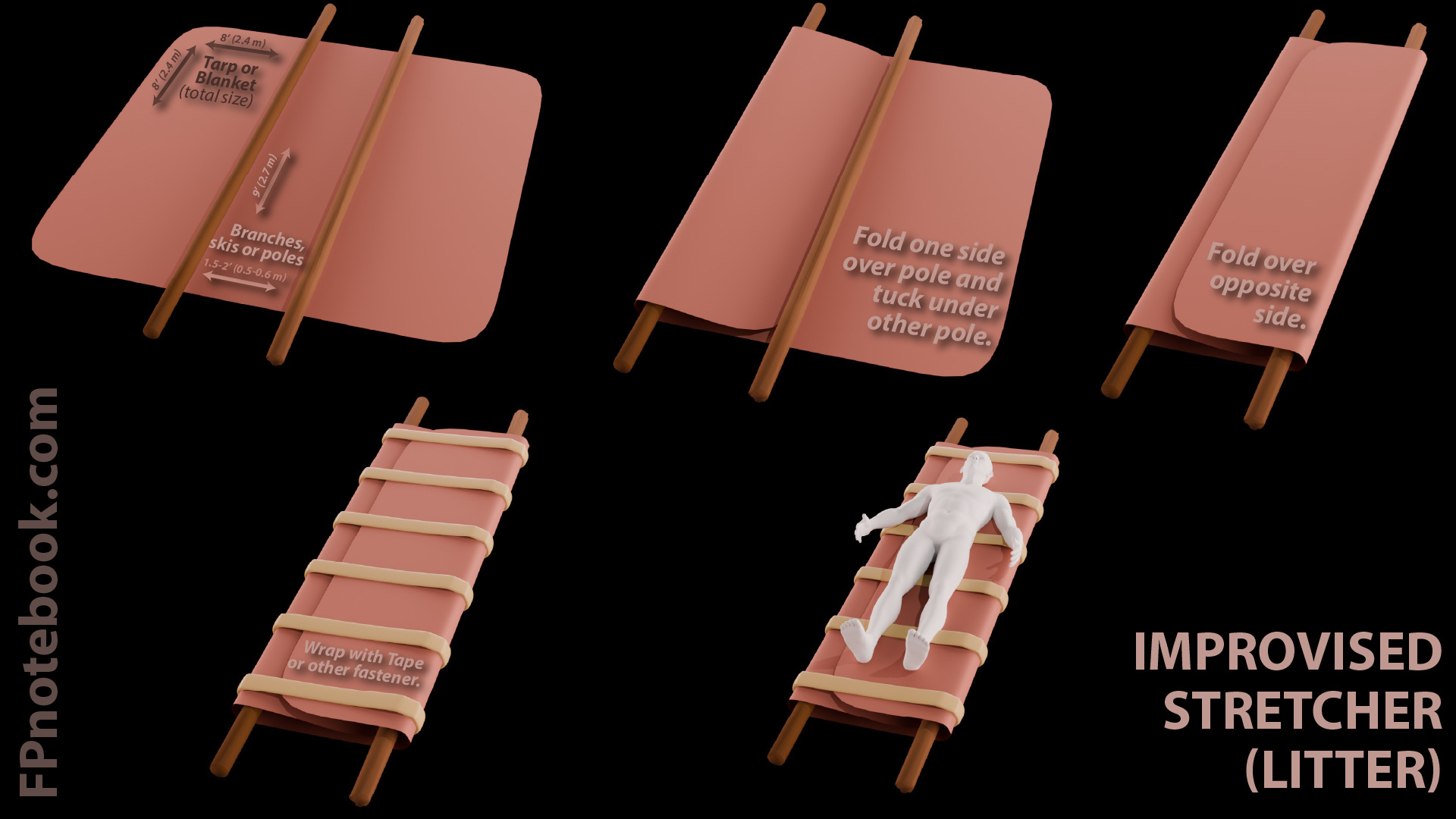
- Improvised litter

- Lay out a tarp or blanket 8 x 8 ft (2.4 x 2.4 M) or combination of two, each 8 ft (2.4 M wide)
- Lay out two rigid 8 ft (2.4 M) skis, branches or poles in parallel, a few inches wider than Shoulder width
- Fold one side of tarp over the top of both poles, then tucked under opposite side
- Fold other side of tarp over the top of pole and overlapping the other tarp side
- Secure the tarp with duct tape, rope or other fastener in ~6 rows evenly spaced along the pole lengths
- Place the litter next to the patient (at or below the patient level)
- Transfer the patient to the litter, maintaining spinal precautions as indicated
- One rescuer at each end of the litter, faces one another and lifts the litter (one rescuer walks backward)
- Keep the stretcher movement even and steady, ideally with a separate leader directing movement and bearer changes
- References
- Auerbach (2007) Wilderness Medicine, Mosby Elsevier
- Lofgran (2019) Crit Dec Emerg Med 33(11):14-5
- Prevention
- Wilderness injury and illness is often preventable
- Basic measures
- Good Hand Hygiene
- Water Disinfection
- Care around boiling water and cooking pots
- Proper disposal of fecal material
- Pre-trip fitness
- Proper footwear
- Protocols
- Resources
- Emergency Communication Devices (e.g. Satellite Messengers, Personal Beacon Locators)
- Outdoor Magazine Review (May 2018)
- Outdoor Gear Lab Review (April 2019)
- Garmin InReach (e.g. InReach Mini, Satellite Messenger)
- References
- Park and Seibert (2019) Crit Dec Emerg Med 33(3):19-25
- Schimelpfenig (2015) Evidence Informed Wilderness Medicine, Wilderness Medicine Institute of NOLS