Transthoracic Echocardiogram, Echocardiogram, Echocardiography, Emergency Echocardiography, Emergency Echocardiogram, Cardiac Ultrasound, Point Of Care Cardiac Ultrasound, Heart POCUS, Cardiac POCUS
- See Also
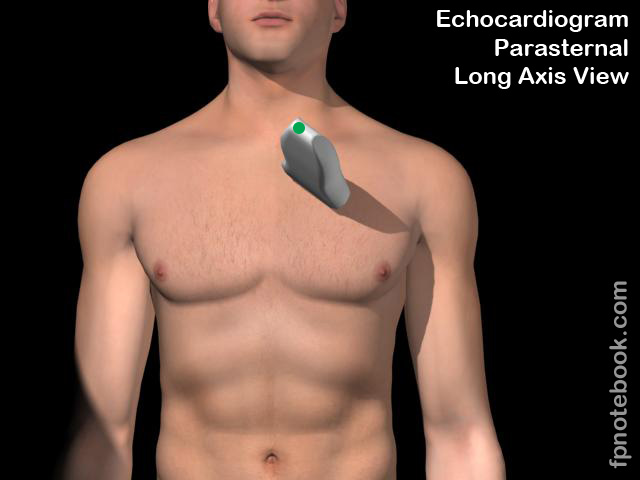
- Parasternal Long-Axis Echocardiogram View ( PLAX View)
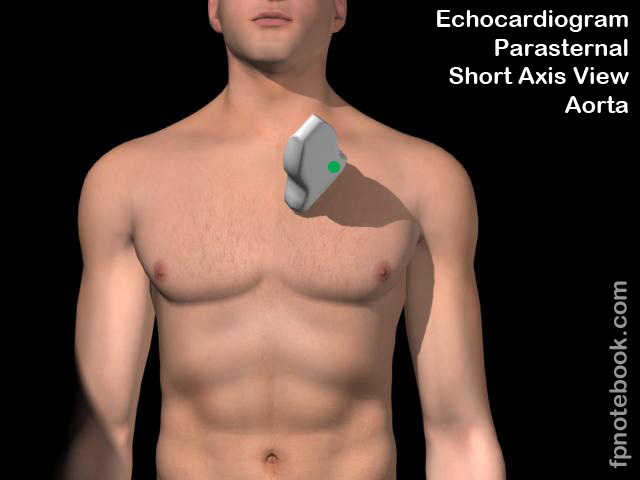
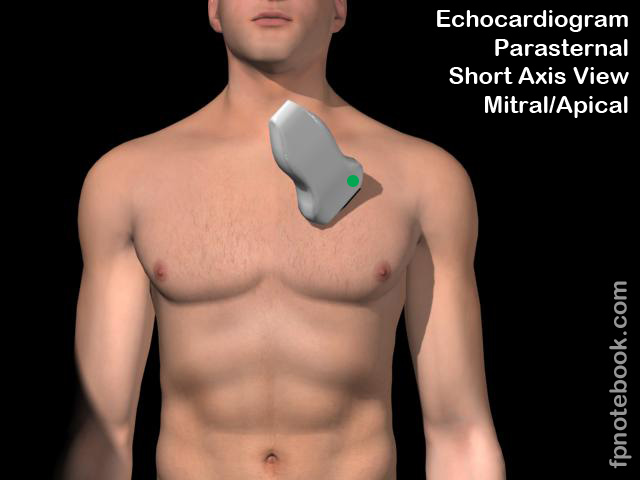
- Parasternal Short-Axis Echocardiogram View (PSAX View)
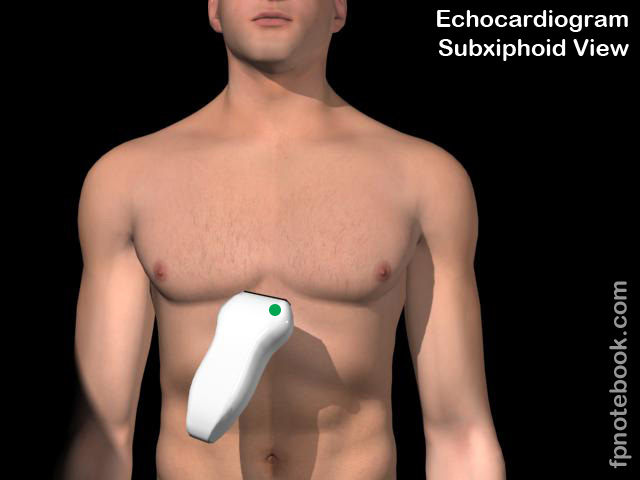
- Subcostal Echocardiogram View (Subxiphoid Echocardiogram View)
- Apical Four Chamber Echocardiogram View
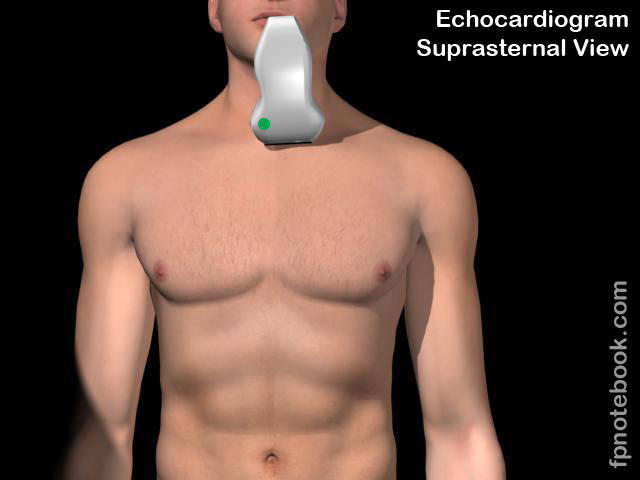
- Suprasternal Echocardiogram View
- Echocardiogram in Congestive Heart Failure
- Inferior Vena Cava Ultrasound for Volume Status
- Emergency Pericardiocentesis
- Pericardial Effusion
- Stress Echocardiogram
- Transesophageal Echocardiogram
- Ultrasound
- Indications
- Emergency Echocardiogram
- Emergency Echocardiography (or Focused Ultrasound Examination) does not replace a complete Echocardiogram
- Emergency Echocardiogram is done to answer specific emergency related questions
- Cardiac Arrest evaluation (echo during pulse checks)
- Pericardial Effusion
- Cardiac activity
- Advanced skills
- Heart wall motion and cardiac contractility
- Valvular abnormalities
- Overall Approach (Mnemonic: 5Es)
- Ejection Fraction (estimate cardiac contractility or EPSS)
- Equality (right heart size in comparison with left)
- Effusion (Pericardial Effusion)
- Entrance (Inferior Vena Cava Ultrasound)
- Exit (aortic root measurement)
-
Cardiac Arrest
- Cardiac standstill
- Evaluate during pulse checks during CPR
- A flicker of heart wall motion beyond mitral valve movement may signal cardiac activity
- Distinguish from Ventricular Fibrillation appearance (shimmering appearance of ventricular wall)
- Distinguish from lung excursion with Positive Pressure Ventilation (stop PPV to visualize heart activity)
- Prolonged cardiac standstill may demonstrate congealed blood in ventricle
- Associated with little to no chance of ROSC and survival (helps direct cessation of code)
- Identify reversible causes of PEA
- Cardiac Tamponade (Pericardial Effusion and right ventricular collapse in diastole)
- Hypovolemic Shock (hyperdynamic heart with with small ventricular chamber)
- Myocardial Infarction (new wall motion abnormality, decreased contractility or EF)
- Pulmonary Embolism (consider empiric PE Thrombolysis)
- See Echocardiogram in PE
- See Focused Lower Extremity Venous Ultrasound
- Acute dilated right ventricular (RV) chamber
- Right ventricle diameter is normally two thirds the left ventricular diameter
- Acute RV dilation findings (contrast with chronic RV dilation of COPD and other Cor Pulmonale)
- Right ventricular free wall thickness <0.5 cm in end diastole
- McConnell's Sign
- Dilated right ventricle with RV free wall akinesis and normal apical contractions
- References
- Swaminathan and Avila in Herbert (2020) EM:Rap 20(5):10
- Cardiac standstill
-
Shock or Hypotension
- See RUSH Protocol
- Acute Dyspnea
-
Pulmonary Embolism
- Evaluate right heart function
- Dilated right ventricle and right atrium (normally smaller than the left ventricle)
- D-Sign (interventricular septum bows into the left ventricle with contractions)
- RV wall will be thin in acute right heart strain (contrast with a thick RV wall in chronic RV strain)
-
Trauma
- See FAST Exam
-
Myocardial Infarction
- Wall motion abnormalities are very challenging to visualize unless severely diminished
- Newer Ultrasound machines and technologies may automate analysis
- Ultrasound-Guided Pericardiocentesis
- Pericardial Effusion (and Cardiac Tamponade)
- Thoracic Aortic Dissection (Type A)
- Background
- Basics
- Probe Direction Indicator
- Issue of confusion on learning Bedside Ultrasound (emergency department and Critical Care)
- Cardiac echo is, by convention, performed with direction indicator on the screen right
- Provider should direct the indicator when transverse to point to 3:00 (not 9:00)
- Ultrasound machines when on cardiac preset
- Automatically move the screen indicator to screen right
- All other regional Ultrasound conventions and machine presets (non-cardiac)
- Automatically move the indicator to screen left (and pointing to 9:00 position)
- Follow simple rule: Probe indicator direction should match the screen indicator direction
- Applies when screen directly in front of operator
- Check the probe indicators screen position
- Observe the screen while tapping or drawing finger across the indicator end
- Use Cardiac Phased-Array transducer (1-5 MHz)
- Use cardiac preset
- Transducer marker corresponds to screen right (contrast with other presets where marker is on screen left)
- Optimize the resolution for the intended depth
- Deeper structures require lower frequency, often labeled as "penetration mode" (lower resolution)
- Superficial structures may be imaged with higher frequency, labeled as "general mode" (and higher resolution)
- Faster frame rate (>20 fps is ideal) to catch dynamic images throughout Cardiac Cycle
- Image as shallow as possible (reduce depth)
- Narrow the sector (narrow the pie shaped wedge of Ultrasound signals)
- Zoom to the area of interest
- Avoid using "gain control" to improve image definition
- Gain control only adjusts "receiver gain" of the signals that are returning to the scan head (1% of those sent)
- Image resolution is based on scan frequency, which is sending signals
- Modifying the "receiver gain" only further degrades the resolution
- Only after optimizing resolution for depth, should the gain control be used to modify the image brightness
- Use the receiver gain only to "darken the snow" or "whiten the landmarks"
- Use cardiac preset
- Heart axis
- Longitudinal refers to long orientation of left ventricle (right Shoulder to left hip)
- Longitudinal view will be more horizontal in obese patients and more vertical in thin, tall patients
- Most patients will have at least one adequate view to visualize heart function
- Technique for a single view can be modified to visualize most structures
- Quality of view may be inversely proportional to body habitus (i.e. Obesity degrades the view)
- However, do not pre-adjust machine settings based on habitus alone
- Some larger patients have excellent cardiac windows with wide open rib spaces
- Subxiphoid Echocardiogram View
- Parasternal long axis
- Apical Four Chamber Echocardiogram View
- May offer a four chamber view, when subcostal view is difficult due to intestinal gas or Obesity
- Cardiac contractility
- Factors
- Systolic function
- Ventricular wall should thicken in systole
- Mitral valve leaflet should closely approach the septum in systole (EPSS, seen on PLAX View)
- Ventricular walls should move symmetrically (best seen in PSAX View)
- Asymmetric wall movement may reflect Myocardial Infarction
- Ejection fraction
- Chamber collapse in systole compared with diastole
- Many modern Ultrasounds will automatically calculate an estimate from Apical View
- Systolic function
- Grading
- Severely reduced (EF<30%)
- Mildly reduced (EF 30-55%)
- Normal (EF 55-65%)
- Hyperdynamic (EF >65%)
- Factors
- Background
- Doppler
- See Doppler Echocardiogram
- Pulsed Wave Doppler (PW)
- Continuous Wave Doppler (CW)
- Color Flow Imaging (Color Doppler Imaging or CDI)
- Views
- General

- Resources
- Virtual Thransthoracic Echo
- Sub-xiphoid View Video (SonoSite)
- Apical 4-Chamber View Video (SonoSite)
- Parasternal Long Axis View Video (Sonosite)
- Parasternal Short Axis View Video (SonoSite)
- Suprasternal Notch View Video (Sonosite)
- Inferior Vena Cava Ultrasound Video (SonoSite)
- Echocardiographer
- References
- Jordan (2019) Cardiac Ultrasound Protocol Manual, Gulfcoast Ultrasound, p 13-22
- Reynolds (2018) The Echocardiographer's Pocket Reference, Arizona Heart Association, p. 323-4
- Palma, Bourque and Jordan (2019) Introduction to Adult Echo Ultrasound Conference, GulfCoast Ultrasound, St. Petersburg
- Mateer and Jorgensen (2012) Introduction and Advanced Emergency Medicine Ultrasound Conference, GulfCoast Ultrasound, St. Pete's Beach
- Noble (2011) Emergency and Critical CareUltrasound, Cambridge University Press, New York, p. 61-88
- Orman, Dawson and Mallin in Majoewsky (2013) EM:Rap 13(1): 4-6
- Reardon (2011) Pocket Atlas Emergency Ultrasound, McGraw Hill, New York, p. 61-106