Parasternal Long-Axis Echocardiogram View, PLAX View, E-point Septal Separation, EPSS, Aorta Diameter Measurement on PLAX View, Aortic Dissection on PLAX View
- See Also
- Echocardiogram
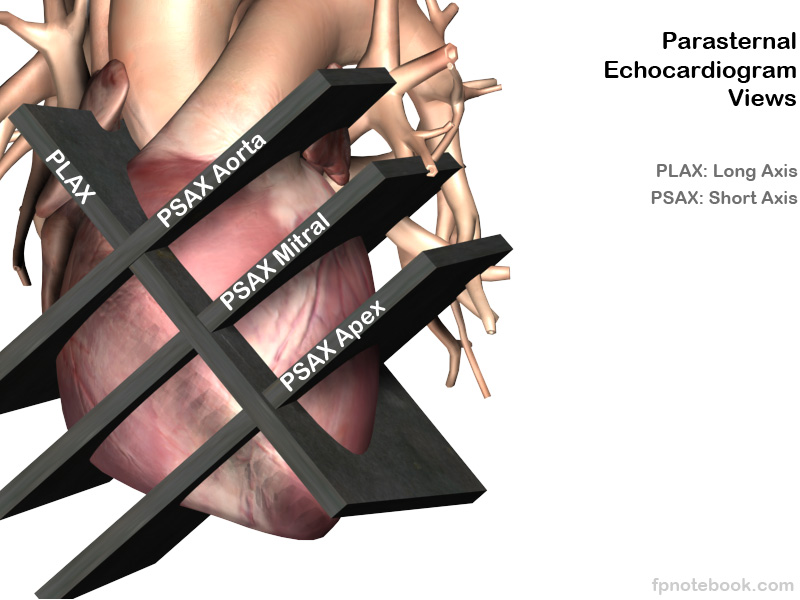
- Parasternal Long-Axis Echocardiogram View ( PLAX View)
- Parasternal Short-Axis Echocardiogram View (PSAX View)
- Subcostal Echocardiogram View (Subxiphoid Echocardiogram View)
- Apical Four Chamber Echocardiogram View
- Suprasternal Echocardiogram View
- Echocardiogram in Congestive Heart Failure
- Inferior Vena Cava Ultrasound for Volume Status
- Emergency Pericardiocentesis
- Pericardial Effusion
- Stress Echocardiogram
- Transesophageal Echocardiogram
- FAST Exam
- Ultrasound
- Background
- Improved window (bring heart closer to transducer and reduce rib shadowing)
- Patient positioned in left lateral decubitus position (if possible)
- Start along sternal border near the 3rd interspace and check several interspaces inferiorly and laterally (to left)
- View improves when patient breathes out
- More difficult view in COPD or Asthma
- Preferred view in Obesity, pregnancy or Ascites (increased abdominal pressure pushes the heart upward into the chest)
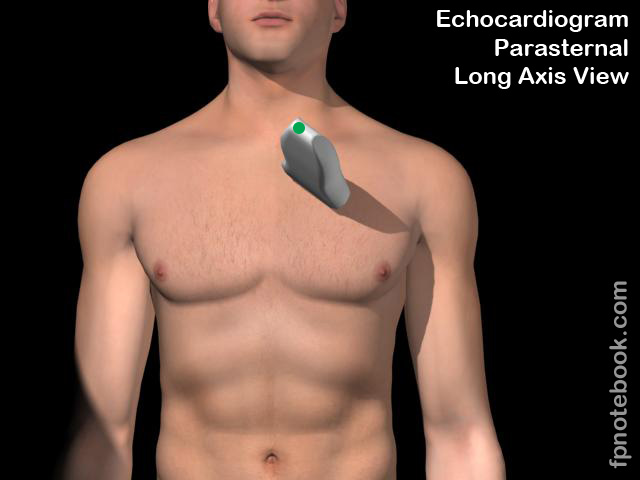
- Transducer orientation
- Transducer 3-5 cm to the left of the left sternal border at the 3rd to 5th intercostal space
- Transducer indicator pointed towards patient's right Shoulder (10:00 position) in cardiac mode
- Technique
- Images
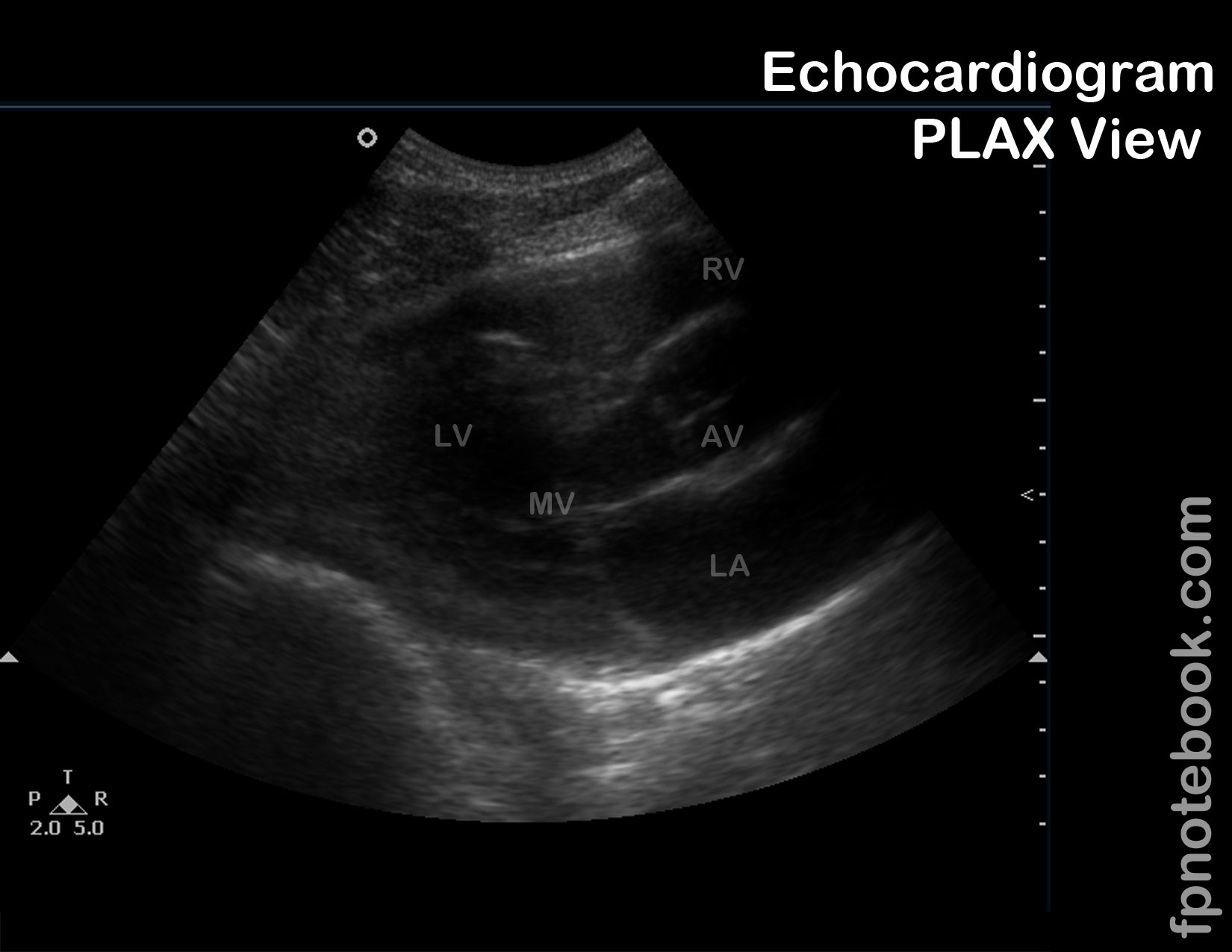
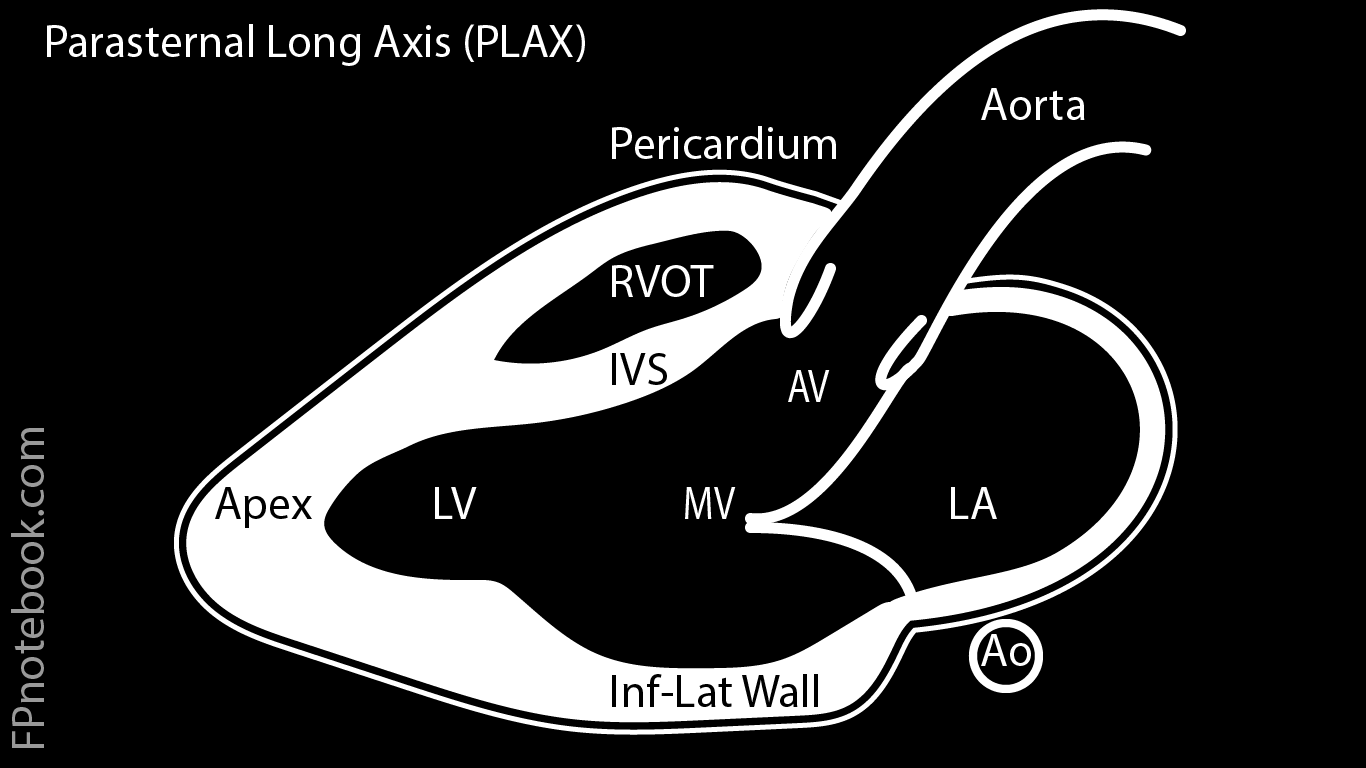
- Standard Parasternal Long Axis (PLAX) Landmarks
- Right ventricle or right ventricular outflow tract
- Left ventricle, aortic valve and proximal aorta
- Mitral valve and left atrium
- Descending Aorta
- Parasternal Long Axis Right Ventricular Inflow Landmarks (tilt toward right hip)
- Right Ventricle
- Tricuspid Valve Leaflets
- Right Atrium and right atrial appendage
- Eustachian Valveand distal inferior vena cava
- Coronary Sinus
- Parasternal Long Axis Right Ventricular Outflow Landmarks (tilt toward left Shoulder)
- Right Ventricular Outflow Tract, Pulmonic Valve and Pulmonary Artery
- Left Ventricle, Mitral Valve and Left Atrium
- Interpretation
- General
- Approach
- Visualizes the positions of the parasternal short axis cross sections (see below)
- Wall motion abnormalities (especially apex and septum)
- Valvular insufficiency (Mitral Regurgitation or Aortic Insufficiency) with color doppler
- Aortic root dilation (best imaged with same probe orientation but at the 3rd intercostal space)
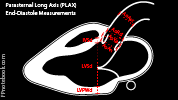
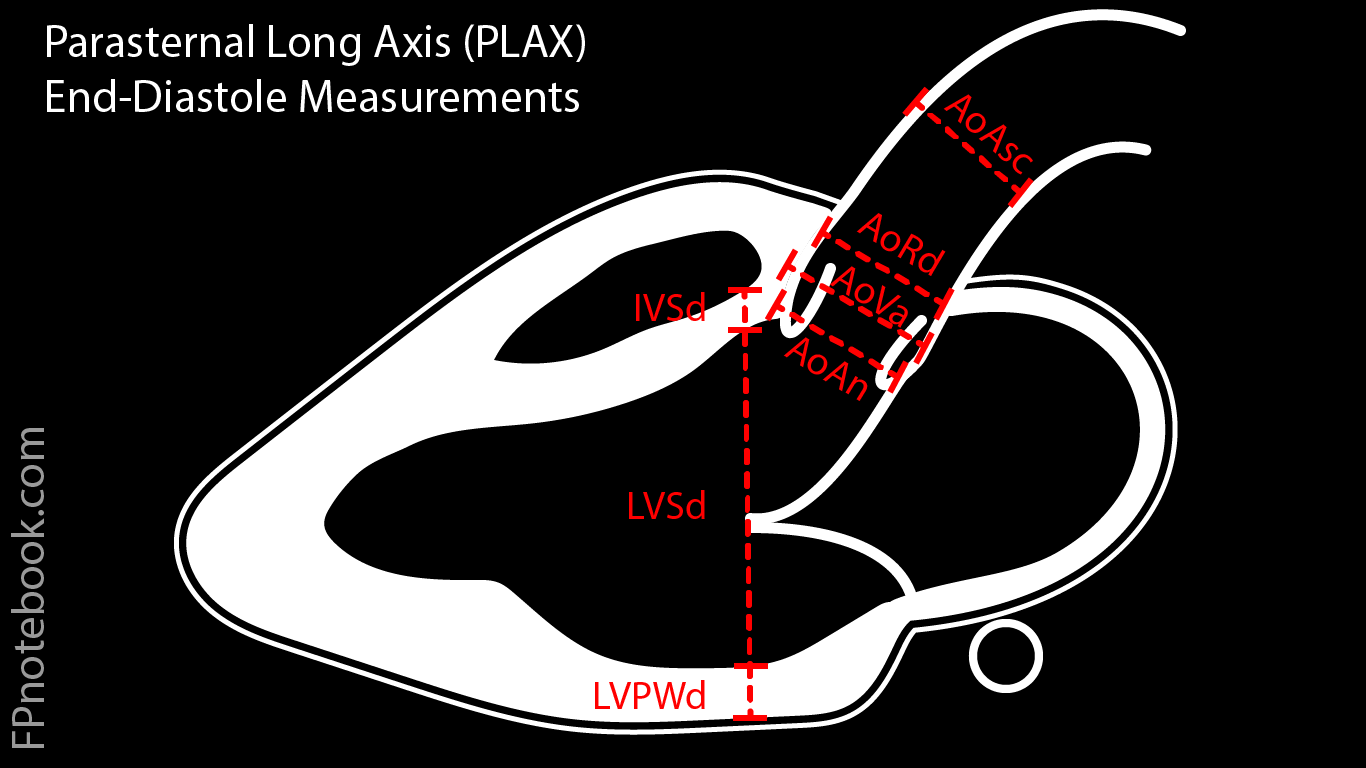
- Measurements: 2D
- End-Diastole (maximal left ventricular dilation, when both aortic and mitral valves are closed)
- Ultrasound machines typically have combined echo measurements
- All three of the following measurements are typically recorded by placing 4 points along a line
- Measure along diagonal line perpendicular to the LV long axis
- Line passes through the end of the closed distal mitral valve tips
- Measure IVSd: Intraventricular Septal width in diastole (immediately below the RVOT)
- Measure LVIDd: Left ventricular internal diameter in diastole
- Measure IVPWd: The inferior (posterior) wall width in diastole (inside the bright pericardial band)
- Measure aortic root diameter
- Measure AoRDd: Aortic root diameter in diastole (leading edge to leading edge)
- Measure ascending aorta (may require shifting up one rib space to visualize ascending aorta)
- The first 3 of these measurements are all considered part of the aortic root
- Measure aortic annulus (normal <=2.6 cm)
- Measure sinus of valsalva (bulge at proximal aorta, origin of coronary arteries, normal <=3.5 cm)
- Measure sino-tubular junction (sinuses of valsalva, normal <=3.4 cm)
- Meaure ascending aorta (normal <=3.4 cm)
- Early-Systole (just as the aortic valves have completely opened)
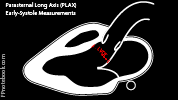
- Measure Left Ventricular Outflow Tract
- Measure LVOT: LV Outflow Tract (inner edge to inner edge)
- LVOT is frequently underestimated
- Measure LVOT: LV Outflow Tract (inner edge to inner edge)
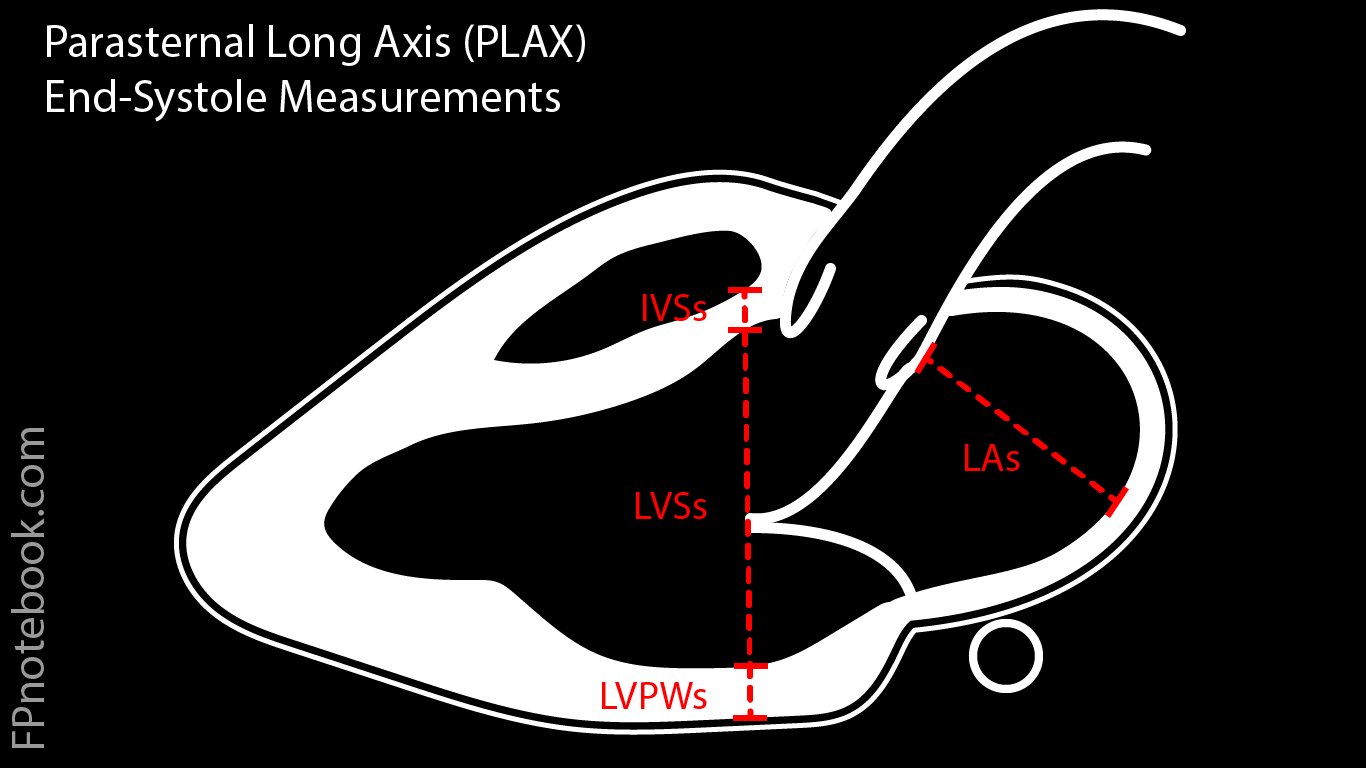
- End-Systole (smallest left ventricle diameter with mitral valves and aortic valves closed)
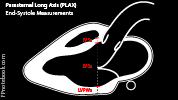
- Measure Left Ventricle Diameter (along same diagonal line perpendicular to the LV long axis measured in diastole)
- Line passes through the end of the closed distal mitral valve tips
- Measure LVIDs: Left ventricular internal diameter in diastole
- Measure Left Atrium Diameter
- Measure LAs: Left atrium (leading edge to leading edge) and starting at aortic sinuses
- End-Diastole (maximal left ventricular dilation, when both aortic and mitral valves are closed)
- Measurements: M-Mode
- Aortic Valve and Aortic Root
- Aortic Root End-Diastolic Diameter (AoRd)
- Anterior aortic root to posterior aortic root (leading edge to leading edge) at end-diastole (lowest point)
- Left Atrial End-Systolic Diameter (LAs)
- Greatest vertical distance (maximal atrial filling) between posterior aortic wall and left atrial wall
- Aortic Valve Systolic Separation (ACS)
- Maximal distance between aortic cusps
- Aortic Root End-Diastolic Diameter (AoRd)
- Mitral Valve
- Appears as 2 peaks, the E point representing diastolic filling and the A point representing the atrial kick
- E-F Slope
- Represents filling of the left the ventricle via the mitral valve
- Normally the E-F slope is relatively steep
- However in Mitral Stenosis it is more flat and the E wave merges into the A wave
- Flattening may also occur in severe Diastolic Dysfunction (noncompliant left ventricle)
- D-E Excursion
- Maximal excursion of the anterior mitral valve leaflet (height of the E Wave)
- E Point Septal Separation (EPSS)
- Distance between the E-point to the lowest intraventricular septum point
- Left Ventricle (measured with line perpendicular to LV long axis through the end of the closed distal mitral valve tips)
- Similar measurements to the 2D left ventricular measurements may be obtained
- End-Diastole (maximal left ventricular dilation, when both aortic and mitral valves are closed)
- Right Ventricular Internal Diameter in end-diastole (RVIDd)
- Intraventricular Septal Diameter in end-diastole (IVSDd)
- Left Ventricular Internal Diameter in end-diastole (LVIDd)
- Left Ventricular Posterior (inferior) Wall Diastolic diameter in end-diastole (LVPWd)
- End-Systole (smallest left ventricle diameter with mitral valves and aortic valves closed)
- Intraventricular Septal Thickness in end-systole (IVSs)
- Left Ventricular Internal Diameter in end-systole (LVIDs)
- Left Ventricular Posterior (inferior) Wall Diastolic diameter in end-systole (LVPWs)
- Aortic Valve and Aortic Root
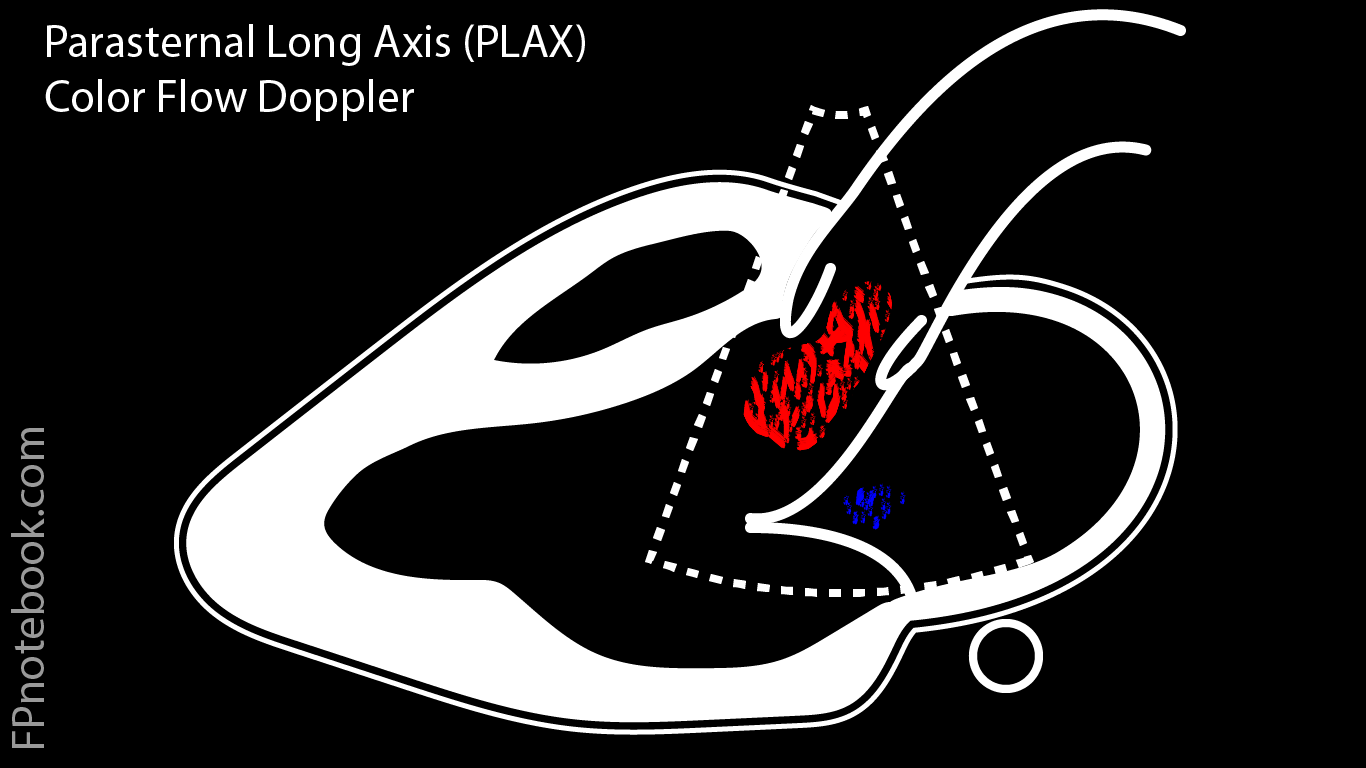
- Visualization: Color Flow Doppler
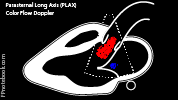
- Standard PLAX View with color directed over both the Aortic valve and Mitral valve regions
- Single view can demonstrate Aortic Regurgitation, Aortic Stenosis, Mitral Regurgitation and Mitral Stenosis

- Interpretation
- Left Ventricular Systolic Dysfunction (CHF)
- Decreased contractility of left ventricle
- Normal
- Depressed or severely depressed
- Hyperdynamic
- Decreased ejection fraction
- Precaution
- PLAX View estimate of EF (fractional shortening) is a less ideal estimate than the apical view biplane method
- The PLAX View-based EF assumes symmetric left ventricular function, allowing for a single point of measure
- Gross Estimate
- Estimate visually what percentage difference is seen between the left ventricle volume in systole and diastole
- M-mode compare end-systolic (ESD) and end-diastolic (EDD) diameters
- Linear calculation: Ultrasound calc package (Fractional Shortening or FS)
- In M-Mode or 2D, measure left ventricle end-diastolic (LVIDd) and end systolic (LVIDs) internal diameters
- Fractional Shortening = 100 * (LVIDd - LVIDs) / LVIDd
- Normal women: 27 to 47% (contrast with normal EF >=55%)
- Normal men: 25 to 43% (contrast with normal EF >=55%)
- Precaution
- Dilated left ventricle (end diastolic diameter >56 mm)
- Measure across widest point between septum and posterior wall
- Chordae tendinae may obscure true posterior wall
- E-point Septal Separation (EPSS) on M-Mode or cine
- Distance between the septum and the mitral valve leaflet when maximally open
- Normal is <8-10 mm (>13 mm is correlated with an EF<30%)
- Aorta Diameter Measurement on PLAX View (for Aortic Dissection)
- Evaluate for Thoracic Aortic Dissection (Type A)
- Obtain Parasternal Long-Axis Echocardiogram View (PLAX View)
- Measure the maximal distance between anterior and posterior walls of aorta
- Probe should be perpendicular to the two aorta walls
- Distance >4 cm is concerning for Aortic Dissection (aortic root is normally 2 to 3.5 cm)
- Other suggestive findings: Pericardial Effusion, flap within the aorta
- Interpretation
- Other findings
- Mitral valve stenosis
- Vitral valve will have a hockey stick appearance at flap distal end (curving away from septum)
- Incomplete opening of the mitral valve septum
- Resources
- Parasternal Long Axis View Video (Sonosite)
- Echocardiographer
- References
- Palma, Bourque and Jordan (2019) Introduction to Adult Echo Ultrasound Conference, GulfCoast Ultrasound, St. Petersburg
- Jordan (2019) Cardiac Ultrasound Protocol Manual, Gulfcoast Ultrasound, p 13-22
- Mateer and Jorgensen (2012) Introduction and Advanced Emergency Medicine Ultrasound Conference, GulfCoast Ultrasound, St. Pete's Beach
- Noble (2011) Emergency and Critical CareUltrasound, Cambridge University Press, New York, p. 61-88
- Orman, Dawson and Mallin in Majoewsky (2013) EM:Rap 13(1): 4-6
- Reardon (2011) Pocket Atlas Emergency Ultrasound, McGraw Hill, New York, p. 61-106
- Reynolds (2018) The Echocardiographer's Pocket Reference, Arizona Heart Association, p. 323-4