Distal Radius Fracture, Colles Fracture, Colles' Fracture, Smith's Fracture, Smith Fracture, Reverse Colles Fracture, Barton's Fracture, Barton Fracture, Hutchinson Fracture, Chauffeur Fracture, Chauffeur's Fracture, Hutchinson's Fracture, Radial Styloid Fracture
- See Also
- Epidemiology
- Most Common Wrist Injury
- Represents one sixth of all Fractures overall
- More common at extremes of age (age<18 years and age>65 years)
- Young (<18 years): High energy injury (e.g. skateboarding, Inline Skating, Downhill Skiing)
- Elderly: Low impact injury (e.g. fall) and underlying Osteoporosis (fragility Fracture)
- Mechanism
- Fall on an outstretched hand
- Exam
- See Forearm Fracture
- See Hand Exam
- See Wrist Exam
- Injury exam mantra: "joint above, joint below, circulation, motor function and Sensation, skin and compartments"
- Evaluate for Open Fracture
- Evaluate for Ecchymosis, deformity, shortening, rotation
- Evaluate Wrist Range of Motion
- Evaluate for Carpal Bone injury (e.g. Navicular Fracture)
- Complete Hand Neurovascular Exam
- Evaluate for Median Nerve injury (finger opposition, Sensation palm and first 3.5 fingers)
- Types
- Colles Fracture
- Occurs with Fall on Outstretched Hand with Forearm pronated
- Transverse Distal Radius Fracture with dorsal displacement and angulation of distal fragment
- "Dinner fork" deformity (distal fragment angulated dorsally)
- Often associated with ulnar styloid Fracture
- Smith Fracture (Reverse Colles Fracture)
- Example Injury: Bicycling Injury with injury when falling over handlebars
- Transverse Distal Radius Fracture
- Volar displacement and angulation of distal radius fragment
- Barton Fracture
- High force injury (e.g. direct blow or motorcycle injury)
- Distal Radius Fracture with dislocation or subluxation of radiocarpal joint
- Colles Fracture or Smith Fracture AND radiocarpal dislocation
- Higher risk injury for Compartment Syndrome and Open Fracture
- Radial Styloid Fracture
- Fracture of the lateral aspect of the distal radius
- Styloid Fractures may be isolated or a part of a larger Distal Radius Fracture
- Styloid Fractures may also be associated with Scaphoid Fractures, carpal dislocations and other Carpal Bone injuries
- Hutchinson Fracture (Chauffeur Fracture)
- Occurs with posterior directed Fall on Outstretched Hand with hand in ulnar deviation
- Intra-articular Radial Styloid Fracture
- Associated with carpal injury (Scaphoid Fracture, lunate Fracture)
- Die Punch Fracture
- Fracture at the Lunate fossa of the distal radius articular surface (50% of radiocarpal joint)
- On impact (e.g. Fall on Outstretched Hand), Lunate punches into the distal radius
- Analogous to a die punch press in manufacturing
- Results in unstable Fracture with intraarticular extension
- Typically requires open reduction and internal fixation (with volar locking plate)
- Uncomplicated, non-displaced Fractures may be treated with non-surgical management
- References
- Kiel (2023) Crit Dec Emerg Med 37(10): 16-7
- Signs
- Distal Radius Fracture
- Displacement ("Dinner Fork" Deformity)
- Dorsal Angulation with volar prominence
- Shortening
- Radial Deviation of hand
- Ulnar styloid Injury often associated (60%)
- Thumb Ulnar Collateral Ligament Injury often associated
- Complications
-
Compartment Syndrome
- Significantly increased pain after reduction despite analgesia may suggest Compartment Syndrome
-
Median Nerve Injury
- Most common nerve injury after angulated, displaced Distal Radius Fracture (esp. Colles Fracture)
- Presents with thumb and index finger Muscle Weakness (test with opposition) and median sensory deficit
- Ligamentous Injury
- Imaging
- Wrist XRay
- See Forearm Fracture
- See Wrist XRay
- Management
- General
- See Forearm Fracture
- External Fracture Reduction as indicated (see below)
- Fracture Immobilization initially with Splinting and then with Casting (see below)
- Orthopedic referral (see indications below)
- Within 3-5 day follow-up if further reduction or surgery otherwise needed
- Colles Fracture
- See Management below
- Smith Fracture (Reverse Colles Fracture)
- Volar angulation of distal radius fragment
- Fracture does not involve articular surface
- Fracture involves articular surface
- Often involves volar subluxation of Carpal Bones
- Open Reduction and Internal Fixation (ORIF)
- Barton Fracture
- Distal Radius Fracture with dislocation)
- Open reduction and Internal fixation (ORIF) required (joint surface is involved)
- Evaluate for Compartment Syndrome, Open Fracture
- Management
- Anesthesia
-
Conscious Sedation
- First-line Anesthesia unless skilled with Hematoma Block or Regional Anesthesia
- Fracture >4 hours prior (Hematoma Block less likely to be effective)
-
Regional Anesthesia
- See Hand and Wrist Regional Anesthesia
- Supraclavicular Brachial Plexus Block
- Infraclavicular Brachial Plexus Block
- Safer, without risk of phrenic nerve injury
-
Local Anesthetic (sufficient if recent Fracture within prior 4 hours)
- Hematoma Block
- Needle inserted dorsally into FractureHematoma
- Aspirate to confirm needle within Hematoma
- Inject 5-10 ml Local Anesthetic
- Inject tip of ulna as well
- Hematoma Block
- Management
- Manual Reduction (Technique 1)
- Assistant Position
- Grasps Forearm for countertraction
- Surgeon Position
- Grasps hand of affected wrist
- Thumb of other hand is placed on distal fragment
- Break up Impaction
- Wrist is hyperextended
- Dorsal Displacement and rotation is corrected
- Apply traction and countertraction
- Continue Thumb pressure on distal fragment
- Distal fragment dorsal cortex apposed with proximal
- Radial and Dorsal Angulation Corrected
- Apply Ulnar and Volar pressure over distal fragment
- Assess if Length is Restored
- Palpate radial styloid
- Management
- Finger Trap Reduction (Technique 2)
- Anesthesia as above
- Break up Impaction by hyperextending wrist
- Place Index finger and thumb in finger traps
- Apply counterweight to upper arm
- Manipulate Fracture as above
- Management
- Immobilization with Sugar Tong Splint
- Fluoroscopy (C-Arm) confirms alignment during Splinting
- Assistant applies steady traction at hand
- Wrist in slight pronation
- Avoid volar flexion of wrist
- Risk of Median Nerve Compression (Carpal Tunnel)
- Apply cast padding from MCP heads to above elbow
- Apply felt pad to volar surface of proximal fragment
- Splint with 10 cm wide, 12 plaster plies around elbow
- Dorsal half ends at MCP heads
- Mold over the distal fragment
- Volar half ends 1-2 cm distal to Fracture
- Maintain wrist in ulnar deviation
- Wrap a strip of plaster around distal splint
- Include distal MCP
- Keep strip proximal to distal palmar crease
- ACE Wrap Sugar Tong in place
- Management
- Isolated Distal Radius Fracture
- Non-displaced Distal Radius Fracture
- See Forearm Fracture in Children (torus Fracture, buckle Fracture, greenstick Fracture)
- Immobilize in a Short Arm Cast for 3 weeks
- Removable splints have been used with similar outcomes to Castingin buckle Fracture (not greenstick Fracture)
- Displaced and overlapping Distal Radius Fracture
- Ulna Fracture also
- See Colles Fracture management above
- Ulna greenstick Fracture
- Complete Ulna Fracture for adequate reduction
- Manage as Colles Fracture
- Ulna intact or greenstick Fracture
- Do not re-Fracture
- Reduction may be quite difficult
- Maximally supinate wrist
- Digital pressure to replace the distal radius
- Alignment is paramount
- Re-align as best as possible
- Apposition is secondary to alignment
- Bayonet apposition is acceptable
- Ulna Fracture also
- Management
- Discharge Instructions
- Management
- Orthopedic Referral Indications
- Images
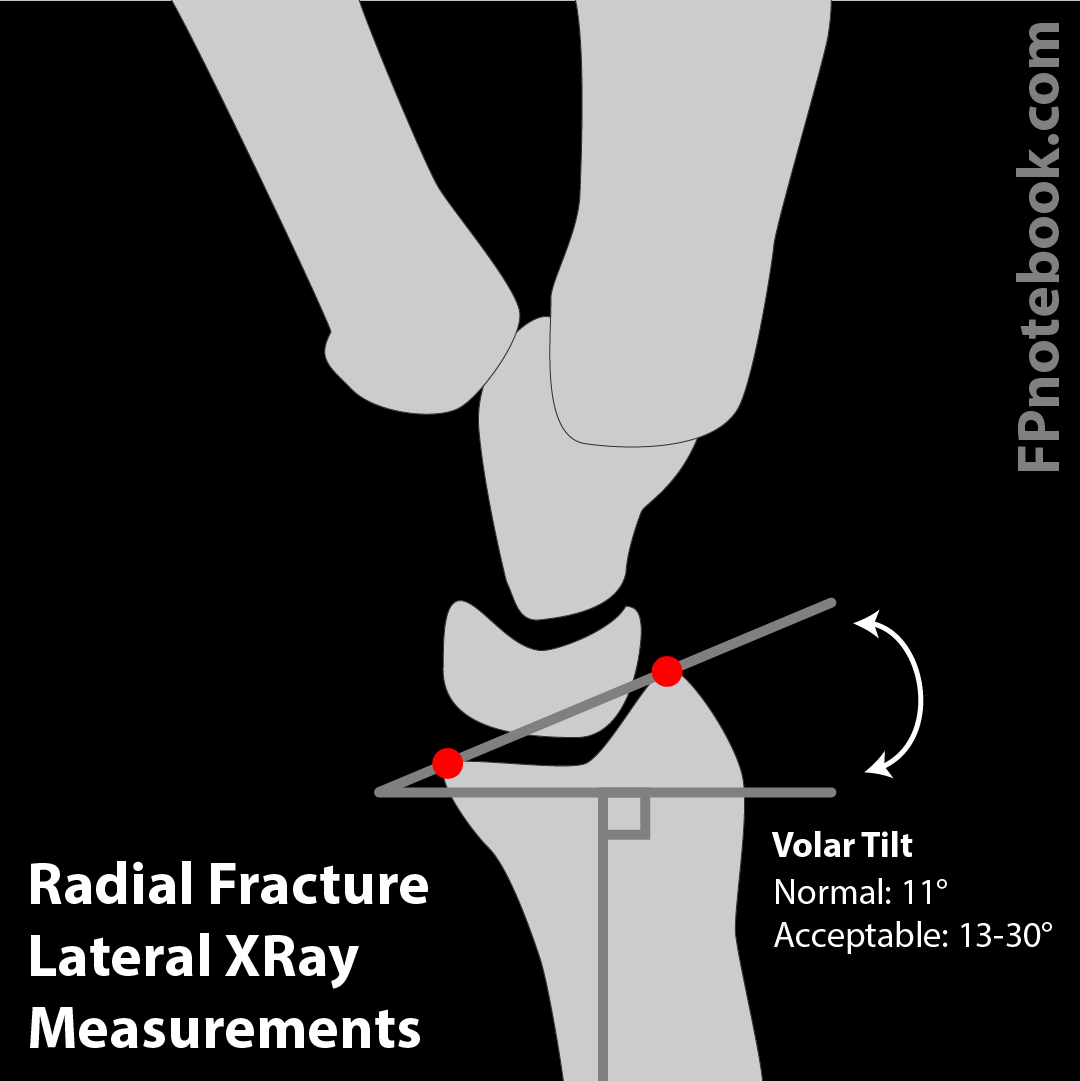
- Distal radius dorsal angulation >5 to 10 degrees
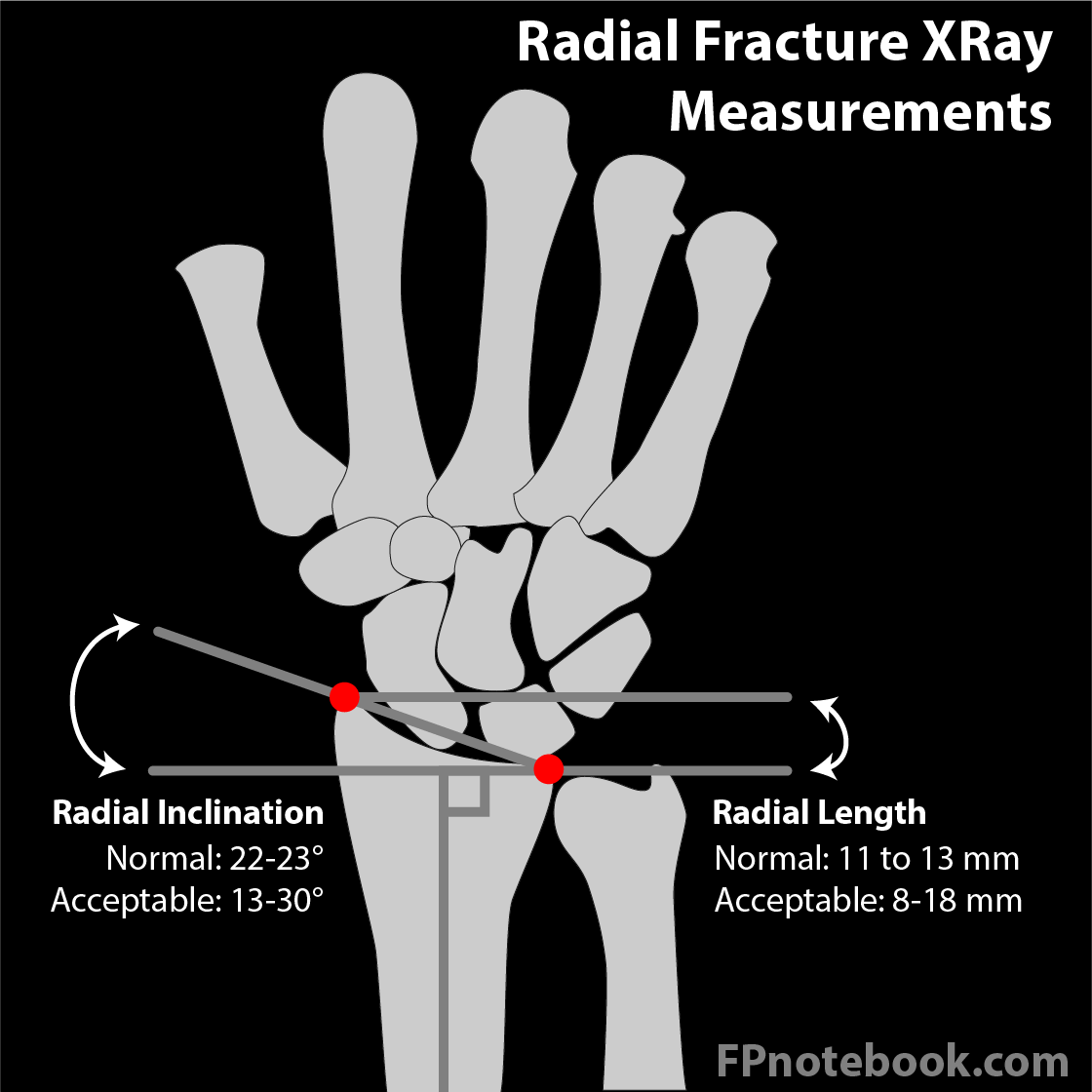
- Distal Radius Measurements
- Line 1 (proximal transverse)
- Draw a horizontal, transverse line across the wrist at the distal aspect of the medial radius (ulna articulation)
- Line 2 (distal transverse)
- Draw a horizontal, transverse line across the wrist at the most distal aspect of the lateral radius (radial styloid)
- Radial length (Radial Height) represents the distance between line 1 and line 2
- Line 3 (Radial Inclination)
- Draw an oblique line between the medial distal radius and the lateral distal radius
- Radial Inclination represents the angle between Line 1 (proximal transverse) and this oblique Line 3
- Line 1 (proximal transverse)
-
Radial Inclination (normal measurements are for adults)
- Normal Radial Inclination: 23.6 +/- 2.5 degrees
- Acceptable inclination: 139-30 degrees
-
Radial Height (radial length) shortening (normal measurements are for adults)
- Normal Radial Height: 11-12 mm
- Acceptable Radial Height: 8-18 mm
- Refer for >2 mm of radial shortening
- Young athletes, or those with occupation or hobby requiring highly functional hand and wrist
- Rotational deformity tolerated (criteria contingent on 50% apposition or greater)
- Age >8 years: Refer for >10 degrees rotational deformity
- Age <8 years: Refer for 15-20 degrees rotational deformity
- Other indications
- Fracture-dislocation
- Carpal Fracture
- Ulnar styloid Fracture
- Unstable Fracture or significantly comminuted
- Radiocarpal or radioulnar ligament injury or instability
- Scaphoid Fracture
- Fracture nonunion
- Epiphyseal Fracture suspected (children)
- Die punch Fracture
- Management
- Follow-Up
- Days 1-2
- Phone: Is Splint too tight?
- Days 5-7
- Repeat Wrist XRay
- Apply Short Arm Cast
- Do not limit motion of the elbow or the metarcarpophalangeal joints
- Anticipate mal-union after swelling decreases
- Elderly
- Mal-union may be acceptable
- Re-manipulation may result in greater morbidity
- Young
- Malunion unacceptable
- Radial head shortening results in dysfunction
- Correction of mal-union
- Re-manipulation and closed reduction
- Open reduction and internal fixation (ORIF)
- External fixator
- Malunion unacceptable
- Elderly
- Week 3
- Non-displaced Fracture follow-up and consider cast removal
- Weeks 4-6
- Cast may be removed
- Weeks 7-9
- Wrist support or cast until pain subsides