Ultrasound-Guided Interscalene Brachial Plexus Block, Interscalene Nerve Block, Brachial Plexus Block, Interscalene Block, Interscalene Brachial Plexus Block
- See Also
- Indications
- Anesthesia to Shoulder, upper arm and clavicle
- Does not provide Anesthesia to ulnar aspect of the Forearm or hand
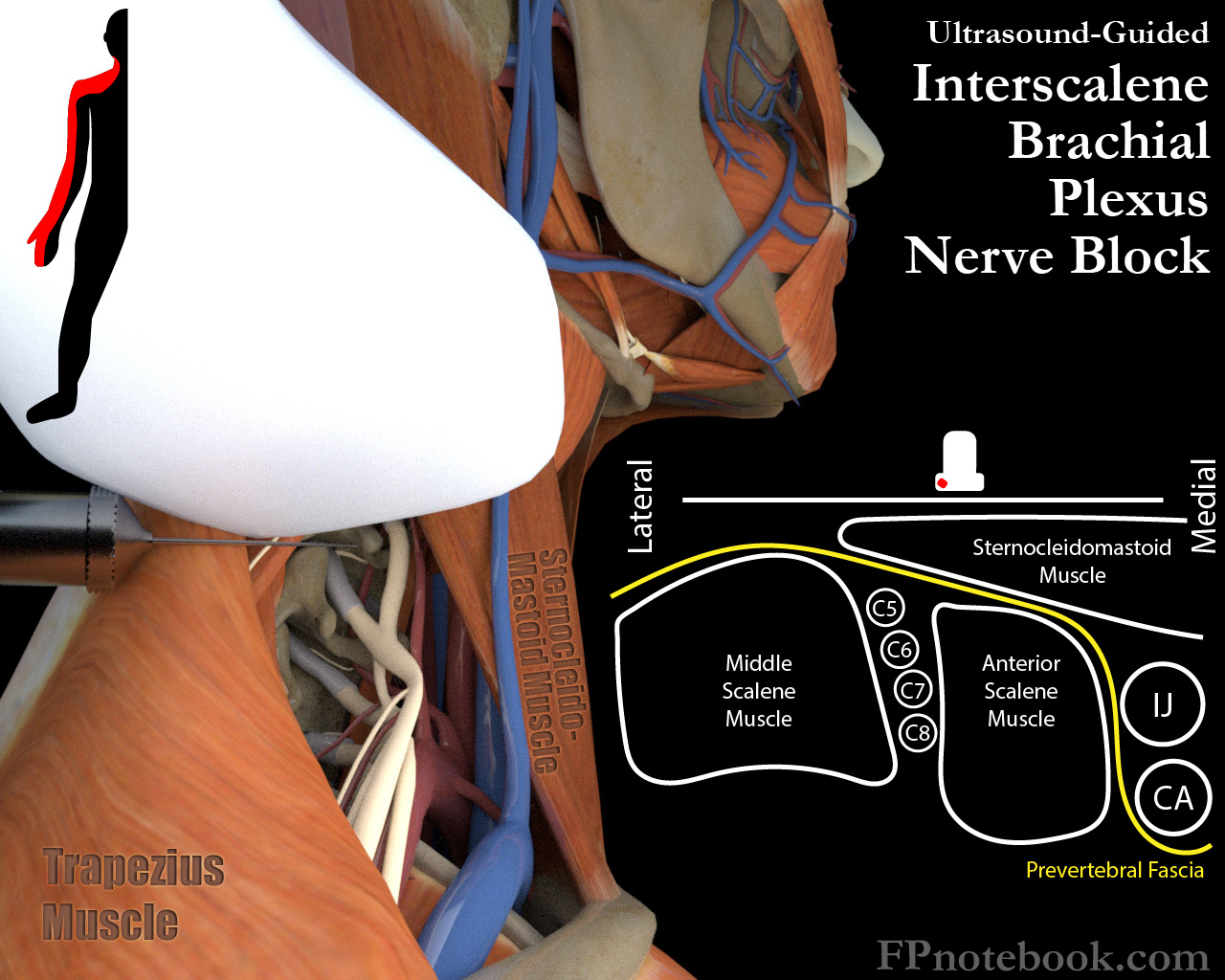
- Anatomy
-
Brachial Plexus Nerve Roots (C5-T1) form the Brachial Plexus trunks and arm Peripheral Nerves
- Brachial Plexus runs 1-3 cm deep in the supraclavicular region, inferolateral to sternocleidomastoid Muscle
- Nerve roots C5-C7 are most accessible to Nerve Block
- Risk of adverse effects on nearby structures
- Carotid Artery and Internal Jugular Vein are medial to injection site
- Phrenic Nerve (transient diaphragm paralysis)
- Superficial Cervical Plexus Block (Transient Horner Syndrome)
- Preparation
- Patient positioning
- Patient lies supine
- Head and neck rotated away from the side of the Nerve Block
- Identify and mark landmarks
- Lateral to Carotid Artery and internal Jugular Vein, posterior sternocleidomastoid Muscle
- Level 2-3 inches (5-7.5 cm) above the clavicle
- Skin Preparation (e.g. Chlorhexidine)
- Drape region
- Sterile covering over Ultrasound high frequency linear probe (sterile gel inside and outside)
- Medication
- Confirm maximum dose for Ropivacaine (or Bupivacaine ) to prevent LAST Reaction
- Ropivacaine 0.5% (preferred over Bupivacaine 0.25% to 0.5%) 7-15 ml
- Syringe 20 ml
- Needle 22 gauge, 2" (5 cm)
- Technique
- Images
-
Ultrasound in Transverse Plane over lateral neck (lateral to Thyroid cartilage)
- High frequency linear probe
- Roughly 2-3 inches (5-7.5 cm) above the clavicle
- Probe overlies posterior aspect of sternocleidomastoid Muscle
- Slide probe laterally until both Carotid Artery and Jugular Vein are visible
- Identify anterior and middle scalene Muscles
- May need to slide laterally to fully visualize the Muscle groups
- Identify Brachial Plexus between the 2 Muscle groups
- Injection Plane
- Inject from lateral to medial
- Under the lateral border of the sternocleidomastoid Muscle
- Target is 1-3 cm deep at the Cervical Nerve Roots (C5-C8)
- C5-C7 Nerve roots will appear as a vertical stop light (3 round stacked nerve-like structures)
- Do NOT inject the actual nerves, only in their vicinity
- Inject from lateral to medial
- Alternatives: Supraclavicular Brachial Plexus Block
- Injection site may be shifted inferiorly to supraclavicular region
- Performed in similar fashion as Interscalene Block
- Only performed under Ultrasound guidance (risk of Pneumothorax)
- Unlike the Interscalene Block, the supraclavicular does not block the Shoulder (only distal to Shoulder)
- Complications
- See Regional Anesthesia
- LAST Reaction (as with any Nerve Block)
- Phrenic Nerve paralysis (common, do NOT perform bilaterally)
- Recurrent laryngeal nerve paralysis (results in Horner Syndrome)
- References
- Warrington (2025) Crit Dec Emerg Med 39(3): 18-9
- Zisquit and Nedeff (2020) Interscalene Block, Stat Pearls, accessed 12/21/2020
- Martel (2020) Regional Anesthesia for Acute Care Conference, attended 12/11/2020
- Ultrasound-Guided Interscalene Brachial Plexus Block, NYSORA, accessed 12/21/2020