Peripheral Nerve Injury, Peripheral Nerve Entrapment, Entrapment Neuropathy, Neuropraxia, Axonotmesis, Axonal Neuropathy, Neurotmesis, Compression Neuropathy, Compressive Neuropathy, Nerve Compression Syndrome
- Definitions
- Categories of Peripheral Nerve Injury
- Neuropraxia
- Least severe Peripheral Nerve Injury
- Myelin fibers surrounding the axon are injured focally
- Axon and connective tissue sheath remain unharmed
- Limited duration of injury (typically days to weeks)
- Axonotmesis
- Axon injury, but preserved connective tissue framework
- Risk of distal nerve degeneration
- Recovery over months to years and frequently incomplete nerve regeneration with residual deficit
- Neurotmesis
- Most severe Peripheral Nerve Injury and least common of the three nerve injury types
- Complete axon disruption, as well as disrupted connective tissue framework
- Normal regeneration of the nerve is uncommon and signficant persistent deficit is the norm
- Pathophysiology
- Mechanisms of nerve injury
- Direct pressure
- Repetitive microtrauma
- Stretch-induced ischemia
- Compression-induced ischemia
- Degree of nerve injury may progress to nerve fibrosis with greater nerve injury
- Severity of injury mechanism
- Duration of exposure to compression or other mechanism
- Causes
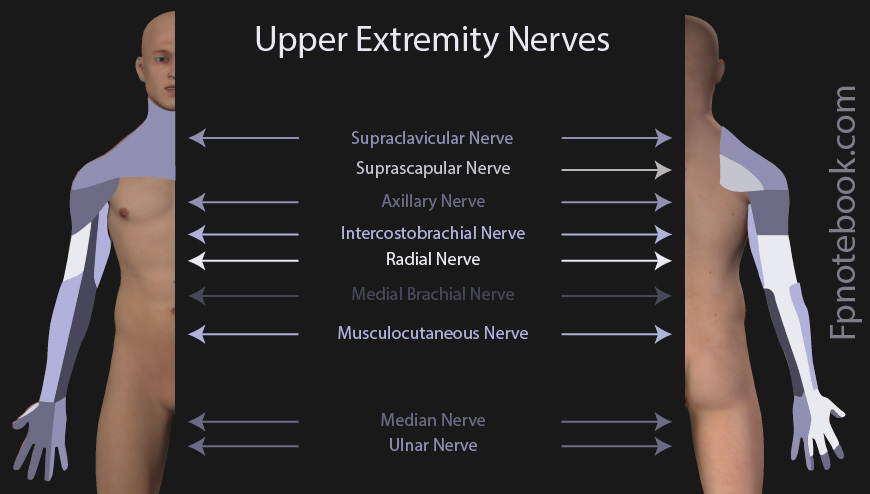
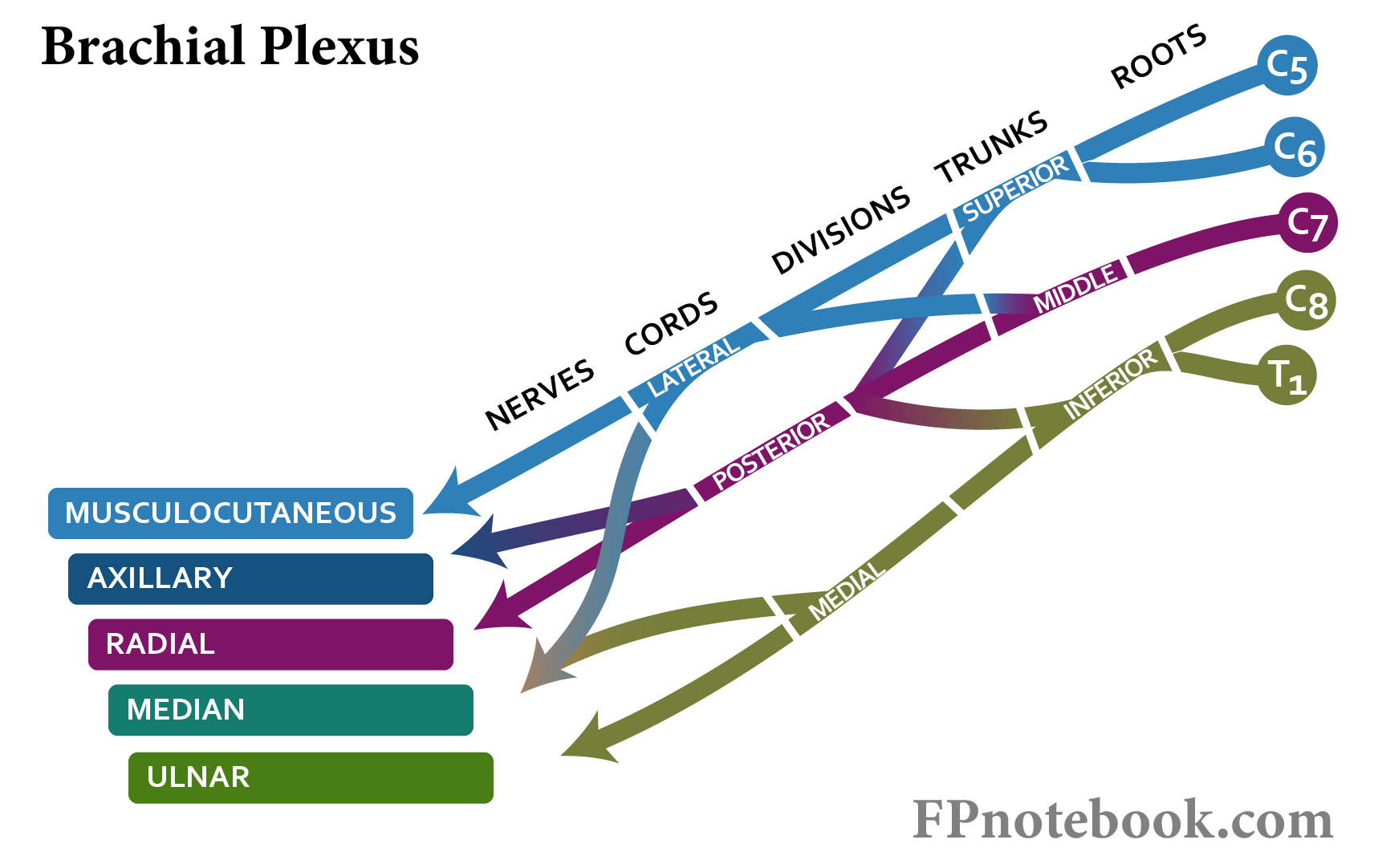
- Upper Extremity
- Images
- Cervical Spine and Cervicobrachial (Axilla)
- Shoulder
-
Humerus
-
Radial Nerve Injury at the Humerus
- Radial Nerve may be compressed in axilla causing Saturday Night Palsy
- Mid-shaft Humerus Fracture may injure Radial Nerve
- Radial Nerve may be entrapped in radial groove
-
Radial Nerve Injury at the Humerus
-
Elbow and Forearm
- Cubital Tunnel (Ulnar Nerve, common)
- Radial Tunnel (and related Posterior Interosseus Nerve Syndrome)
-
Wrist and Hand
- See Overuse Syndromes of the Hand and Wrist
- Carpal Tunnel Syndrome (Median Nerve, very common)
- Ulnar Tunnel Syndrome (Cyclist's Palsy)
- Handcuff Neuropathy (Radial Nerve)
- Causes
- Lower Extremity

- Causes
- Miscellaneous
- Images
- Face
- Secondary Complications
- History
- See Neuropathy
- Musculoskeletal Injury or Trauma to affected region
- Course of symptoms
- Provocative activities
- Exam
-
Musculoskeletal Exam of affected region
- Joint range of motion
- Specific joint exam for region
-
Neurologic Exam
- See Motor Exam
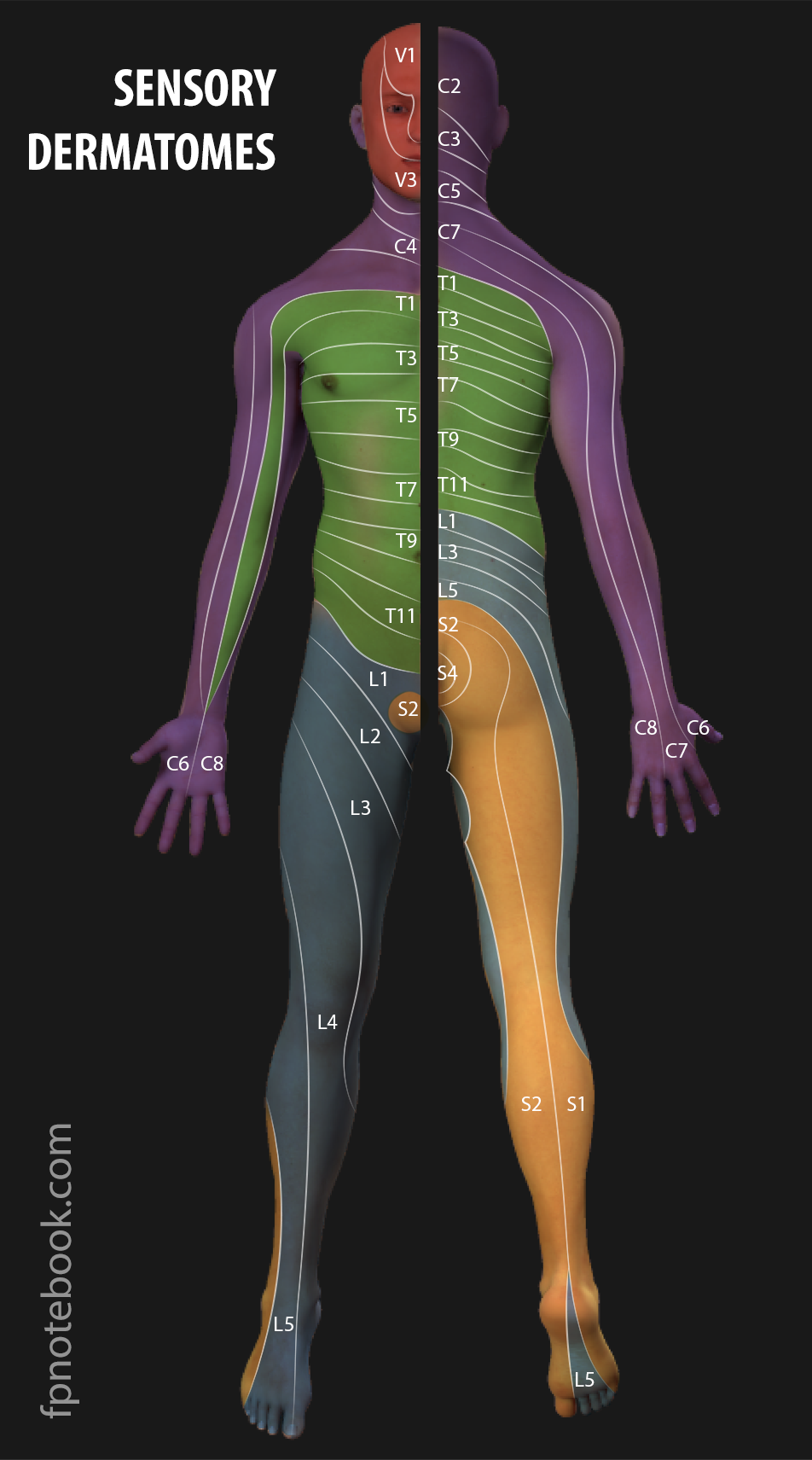
- See Sensory Exam
- See Deep Tendon Reflex
- Symptoms
- Burning pain
- Numbness
- Paresthesias
- Motor Weakness
- Differential Diagnosis
- See Peripheral Neuropathy
- See Mononeuropathy
- Imaging
- See Peripheral Neuropathy
- Modalities
- Ultrasound
- Real-time (point-of-care) evaluation of compression sites that reproduce symptoms
- Directed Corticosteroid Injection for certain compression neuropathies
- Magnetic Resonance Imaging (MRI)
- Ultrasound
- Indications
- Severe weakness
- Multiple nerves involved
- Refractory course to 6-8 weeks of specific conservative therapy
- Diagnostics
- Electrodiagnostic Testing
- See Peripheral Neuropathy
- Modalities (typically performed together)
- Indications
- Localization of nerve lesion in atypical presentations
- Monitoring of nerve injury progression during management
- Presurgical planning
- Management
- See Peripheral Neuropathy
- Initial conservative therapy is preferred for most non-Traumatic compression neuropathies
- Management is specific to the Neuropathy
-
General conservative measures
- Patient Education regarding likely diagnoses and causative factors
- Relative rest with activity modification
- Consider bracing or Splinting (with care not to further compress underlying nerve)
- Consider physical therapy
- Surgical Management
- Indicated in refractory cases
- Lack of full resolution with surgery is common
- Surgical options depend on specific Neuropathy
- Nerve Decompression
- Surgical exploration for underlying cause
- Nerve transfer