Central IV Access, Central Line, Central Line Placement, Central Venous Cetheterization, Central Line Management, Central Line Occlusion, Central Line Complication, Misplaced Central Venous Catheter, Malpositioned Central Venous Catheter, Venous Catheter Site Bleeding, Woggle Technique for Catheter Site Bleeding, Retained Guidewire in Central Venous Catheter Placement, CVC Placement
- See Also
- Indications
- Medications causing tissue necrosis on extravasation or otherwise harmful via peripheral IV
- Large volume infusion required
- Hemodialysis
- Unobtainable or unreliable Intravenous Access
- Pulmonary artery pacing
- Invasive Monitoring
- Right Ventricular Filling Pressures (Central Venous Pressure) and oxygenation (ScvO2)
- Left ventricular filling pressure (pulmonary artery catheter or wedge pressure)
- Contraindications
- General
- Patient refusal
- Uncooperative or agitated despite sedation
- Deep Vein Thrombosis in affected vessel
- Overlying skin abnormality or distorted anatomy
- Prior radiation or surgery distorting or scarring insertion site
- Inability to lie in Trendelenburg position (IJ, SVC; consider Femoral Line instead)
- Contralateral Pneumothorax (IJ, SVC; place on same side as Pneumothorax)
- Ipsilateral AV graft (e.g. Hemodialysis fistula)
- Adequate alternatives are available (e.g. large bore peripheral IV)
- Contraindications
- Significant Coagulopathy
- Precautions in CVC Placement for coagulopathic patients
- Use real-time POCUS guidance (observing the needle from skin to vessel entry)
- Compressible vessels are preferred
- Use the smallest bore needles
- Most experienced operator should perform the line placement
- Safe without reversal IF Compressible site (e.g. IJ, femoral vein inferior to inguinal ligament) AND
- PTT <1.5 x UpperLimitNormal
- INR <3.0 in patient on Warfarin
- Platelet Count >20k
- Antiplatelet agents (e.g. Clopidogrel)
- Direct Oral Anticoagulants (DOAC)
- Safe without reversal IF Non-Compressible Site (e.g. subclavian vein) AND
- PTT <1.5 x UpperLimitNormal
- INR <2.0 in patient on Warfarin
- Platelet Count >50k
- Serum Creatinine <6 mg/dl (or consider with DDAVP)
- References
- Rutherford (2025) Anatomy of Central Venous Access, Hospital Procedures Course, attended 9/12/2025
- Risk Factors
- Mechanical Complications of CVC Placement
- Inexperienced operator
- More than 3 attempts at line placement (RR 6)
- Extremes of weight (BMI <20 or BMI > 30)
- Dehydration
- Large catheters
- Coagulopathy (see above)
- Prior central venous catheter in the same vein
- References
- Rutherford (2025) Anatomy of Central Venous Access, Hospital Procedures Course, attended 9/12/2025
- Preparation
- Informed Consent (patient or surrogate)
- Confirm Identity (verbally and with ID Band, Name, DOB)
- Review Patient History
- Anticoagulants (e.g. DOAC, Warfarin, therapeutic Enoxaparin, Fondaparinux)
- Antplatelets agents (Aspirin, Platelet ADP Receptor Antagonist such as Clopidogrel)
- Review Patient Labs
- Platelet Count
- PT/INR and PTT
- Blood Urea Nitrogen (Uremia with high BUN causes Coagulopathy)
- Equipment
- Skin antiseptic (e.g. Chlorhexidine, Povidone-Iodine, see above)
- Lidocaine 1%, syringe and needle for injection
- Introducer needle, slip tip syringe for guide wire insertion
- Dilator
- Seldinger guide wire
- Scalpel (#11 Blade)
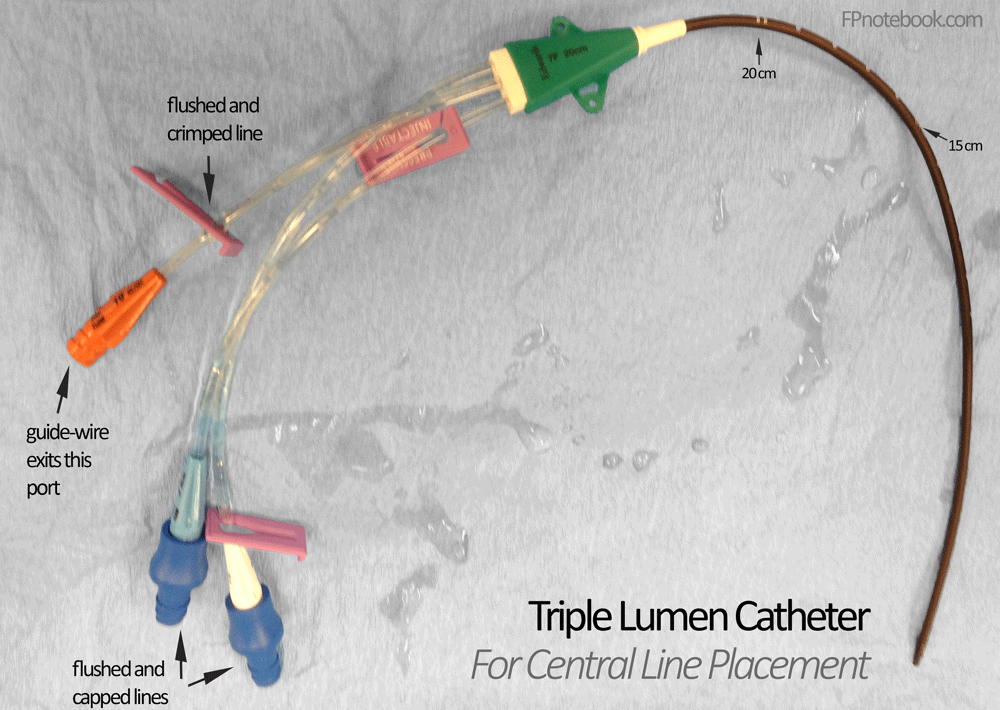
- Triple Lumen Catheter (flush each line with sterile saline)
- Ultrasound with high frequency linear probe (and sterile probe covers with sterile gel)
- Perform under dynamic Ultrasound guidance
- Advantages
- Confirms vessel location and patency
- Real-time confirmation of vessel cannulation
- Decreases the number of access attempts
- Decreases the time to central vein catheterization
- Decreases central access complication rate
- Probe orientation (transverse and longitudinal have similar success rates)
- Transverse probe orientation
- Base needle entry distance from Ultrasound probe based on target vessel depth
- At 45 degree angle, entry distance = depth (e.g. 2 cm depth, 2 cm distance)
- At 30 degree angle entry distance = 1.7 x depth (e.g. 2 cm depth, 3.4 cm distance)
- Follow the needle tip as it is advanced toward the target vessel
- Slide the transverse oriented probe with the needle as it approaches the vessel
- Losing track of the needle tip risks needle malpositioning (esp. too deep)
- Base needle entry distance from Ultrasound probe based on target vessel depth
- Longitudinal probe orientation (indicator toward provider)
- Allows for visualization of needle along entire course
- Start in transverse orientation to identify vein and compressibility, and then rotate 90 degrees
- Risk of probe sliding laterally off vein on onto artery (caution!)
- Transverse probe orientation
- Advantages
- Estimate catheter insertion depth
- Initial guidewire insertion: 20 cm is sufficient in adult
- Right internal Jugular Vein (or right subclavian): Height (cm)/10
- Left internal Jugular Vein (or left subclavian): Height (cm)/10 + 4 cm
- Perform under sterile conditions to reduce infectious complications (i.e. CLABSI)
- Hand Hygiene (Hand Washing immediately before procedure)
- Mask, cap, sterile gown and sterile gloves
- Everyone in room within vicinity of procedure should wear a cap and mask
- Skin Preparation
- Chlorhexidine (preferred)
- Scrubbed back and forth vigorously, and must dry for 3 minutes before skin puncture
- Includes Chloraprep (Chlorhexidine gluconate and Isopropyl Alcohol)
- Povidone-Iodine (Betadine)
- Must dry for 5 minutes before skin puncture
- Chlorhexidine (preferred)
- Large sterile drape to cover entire patient
- Antimicrobial Dressing at catheter insertion site
- Sterile transducer sleeve around Ultrasound probe and cord
- Line insertion pearls
- Use Ultrasound guidance (see above)
- Approach vessel from a shallow angle (e.g. 30 degrees, maximum of 45 degrees)
- Stabilize needle and syringe on entering skin to prevent too forceful and deep initial needle entry
- Once blood enters syringe, stabilize needle with 3 three fingers against patient and remove needle
- Prevents needle exiting vessel while removing syringe
- Alternatively, an angiocatheter large enough to pass guidewire may be used for initial vessel entry
- On passing seldinger guidewire, the curve in guidewire should be directed toward heart (midline)
- Dilator insertion should parallel the needle entry angle (typically shallow)
- Twist the dilator as it enters vessel to ease venous catheter insertion
- On confirmation of line placement, aspirate each line
- Approach
- Site Selection in stabilized patients
- Precaution
- Site selection should avoid sites with overlying infection, altered anatomy, Trauma or distortion
-
General patient without other risk factors
- Internal Jugular Central Line is preferred (lowest risk site)
- Avoid Femoral Central Line overall (aside from codes) due to the highest rate of complications (DVT, infection)
- Consider alternatives to central access
- Morbidly obese
- Subclavian Central Line is preferred
- Internal Jugular Vein landmarks are typically difficult to localize in the morbidly obese
- Avoid femoral vein Central Line due to infection risk
-
Pneumothorax or Hypoxemia
- Internal Jugular Central Line is preferred, placed on ipsilateral side of Pneumothorax
- Avoid Subclavian Central Line (unless on same side as the Pneumothorax)
-
Coagulopathy (increased bleeding risk such as Hemophilia, Thrombocytopenia)
- Internal Jugular Central Line is preferred
- Avoid Subclavian Central Line as it is a noncompressible site
-
Hypercoagulable state (increased thrombosis risk)
- Subclavian Central Line is preferred
- Avoid Internal Jugular Central Line (highest risk site for DVT)
- Approach
- Site Selection by circumstance
- Crashing patient (Code, CPR) or Trauma patient (C-Spine Immobilization)
- Intraosseous Access
- Femoral Line
- Replace with supraclavicular line (IJ, EJ, Subclavian) when stabilized
- Children
- Femoral Line (if intraosseous fails)
-
Central Venous Pressure monitoring or Sepsis catheter
- Supraclavicular line (IJ, EJ, Subclavian)
- Approach
- Pediatric Patients
- Central catheter sizes in children
- Infant: 3 French (24 gauge)
- Toddler/Preschool: 4 French (20 gauge)
- School age: 5 French (18 gauge)
- Catheter placement pearls
- Sedation allows for procedure (e.g. Ketamine 4 mg/kg IM)
- May use introducer (catheter over needle only) for initial Resuscitation
- May later, use guidewire through introducer catheter to place standard Central Line
- Catheter wire kinking, looping or fracturing (or dilator displacement)
- Gently move the wire in and out of dilator while dilator is being advanced
- Dilator misdirected down divergent path
- Rotate the dilator while inserting through subcutaneous tissue
- References
- Claudius, Behar, Chang and Santillanes in Herbert (2016) EM:Rap 16(4): 3-4
- Claudius, Behar and Hofmann, Santillanes, Bowman in Herbert (1018) EM:Rap 18(6):13-4
- Approach
- Securing Central Line and Maintenance
- Line holders
- Apply the white (inner) and blue (outer) line clips at 2 cm from the skin entry site
- One hole for Suture on each side of the clamp
- Apply the antimicrobial, bio-patch under the line at the skin entry site (with blue side of patch up)
- Proximal attachment (at base of the triple lumens)
- One hole for Suture on each side
- Suture the line in place
- Anesthetize the skin at each of the four Suture holes
- Use a 2-0 Silk Suture with curved needle (typically not in the Central Line kit) and needle driver
- Apply a sterile, transparent Occlusive Dressing over the Central Line entry
- Skin entry site and bio-patch should be clearly in view
- Triple lumen ports will exit at the notch in the Occlusive Dressing
- A second Occlusive Dressing with wings is applied beneath the ports to further secure line
- Apply the white (inner) and blue (outer) line clips at 2 cm from the skin entry site
- Mark the entry
- Using a marker on the Occlusive Dressing, write the date, time and provider initials
- Maintenance
- Check Central Lines daily for signs of infection
- Change Central Lines at 10 days or at signs of infection
- Consider Central Line removal when not used for >1 day
- Preparations
- Devices
- Triple lumen catheter (typical Central Line)
- Double lumen catheter
- Hemodialysis catheter
- Cordis catheter
- Indicated for Hemodialysis or critically ill patients requiring advanced hemodynamic monitoring
- Complications
- General
- Catheter Related Bloodstream Infections (CRBI)
- Collateral injury to surrounding structures
- Pneumothorax (IJ, EJ, Subclavian Line)
- Bladder or retroperitoneal injury (Femoral Line)
- Immobilization-related effects
- Deep Vein Thrombosis (especially Femoral Line)
- Other cardiovascular-related effects
- Air Embolus
- Pre-flush all catheters with saline
- Perform in trendelenburg position (both CVC Placement and removal)
- Perform needle entry during patient expiration
- Ensure adequate patient hydration
- Hold thumb over introducer needle while readying to insert guidewire
- Confirm that all catheter ports are clamped or capped
- Syringe handles should be upright (bubbles rise away from syringe tip)
- Cardiac Dysrhythmia (esp. Atrial Fibrillation; VT may occur)
- Normalize Electrolytes if possible before CVC Placement (esp. Potassium and Magnesium)
- Observe patient on cardiac monitor during line placement
- Limit guidewire insertion to no more than 20 cm
- If Arrhythmia occurs, promptly withdraw guidewire to safe distance (out of atrium)
- Air Embolus
- Retained Central Catheter Guidewire
- Unrecognized at time of procedure in up to one third of cases
- Missed on post-procedure imaging while focused on other features (e.g. IV position, excluding Pneumothorax)
- Unrecognized in some cases for up to years after procedure
- Delayed diagnosis risks serious complications
- Dysrhythmias
- Cardiovascular injury
- Venous Thrombosis
- Cardiac Tamponade
- Death
- Removal
- Typically requires Intervention Radiology for wire retrieval under fluoroscopy
- If guide wire is still partially encased in IV catheter, negative pressure technique may be attempted
- Repeatedly aspirate from catheter to attempt drawing wire back into channel toward skin surface
- When wire reaches skin level, a clamp may be applied to catheter (and wire within), and both withdrawn
- References
- Broder (2023) Crit Dec Emerg Med 37(10): 18-20
- Unrecognized at time of procedure in up to one third of cases
- Central Line Occlusion
- Attempt to flush the line with saline first
- Alteplase (tPA) protocol
- Reconstitute 2 mg vial of Alteplase in 2 ml Normal Saline
- Instill 2 ml Alteplase solution into clotted port
- Wait 30 minutes, then attempt to aspirate blood
- If no blood aspirated, wait another 90 minutes and attempt aspiration again
- If still no blood aspirated after first tPA instillation
- Repeat instillation of another 2 ml Alteplase
- Reattempt aspiration at 30 and 90 minutes as above
- If able to aspirate blood
- Aspirate 5-10 ml blood and discard
- Irrigate catheter with multiple Normal Saline flushes
- References
- Complications
- Site Specific Risks (may direct site selection)
- Precautions related to Complication Rates
- Overall CVC Complications have decreased significantly in the last 20 years
- Site specific complications have also decreased significantly
- Reduced complication rates are largely related to mitigating risks
-
Internal Jugular Central Line
-
Deep Vein Thrombosis (DVT)
- As of 2020, all Central Lines (IJ, femoral and subclavian) all have similar DVT Risk (3-3.5 per 1000 catheter days)
- Previously >2 fold increased risk over Subclavian Central Line
- Timsit (1998) Chest 114: 207-13 [PubMed]
- Parienti (2015) N Engl J Med 373(13):1220-9 [PubMed]
- Infection risk (CLABSI)
-
Deep Vein Thrombosis (DVT)
- External Jugular Central Line
- Failed placement
- Pneumothorax
-
Subclavian Central Line
-
Pneumothorax (highest risk site)
- Pneumothorax risk was 1-3% in 2002 (and similar risk in 2020)
- Noncompressible (uncontrolled bleeding risk)
- Infection risk (CLABSI)
-
Deep Vein Thrombosis (DVT)
- As of 2020, all Central Lines (IJ, femoral and subclavian) all have similar DVT Risk (3-3.5 per 1000 catheter days)
-
Pneumothorax (highest risk site)
-
Femoral Central Line
- Deep Vein Thrombosis (DVT)
- Infection risk (CLABSI)
-
Arterial Puncture
- Risk 6-7% in 2002 (contrast with 3% for IJ and 0.5% for subclavian vein)
- Children
- Preferred site in children (lower risk than IJ)
- Overall Complications
- Femoral Lines now had similar risks to internal jugular: infection rate (1.2%), thrombus rate (1.4%)
- Femoral also had the lowest failed placement rate (5%) compared with 9% IJ and 15% subclavian
- Parienti (2015) N Engl J Med 373(13):1220-9 [PubMed]
- Reduced CVC duration (2-6 days) has significantly reduced complications
- Femoral Lines specifically have an average duration of 2.7 days
- Remove the Central Line as soon as Peripheral IV Access is suffiicient
- Casanegra (2011) J Hosp Med 6(1):33-6 +PMID: 20578050 [PubMed]
- Femoral Lines now had similar risks to internal jugular: infection rate (1.2%), thrombus rate (1.4%)
- References
- Complications
- Misplaced or Malpositioned Central Venous Catheter
- Background
- Central venous catheter (CVC) is considered malpositioned if its tip is not in the superior vena cava or right atrium
- Mild catheter tip migration is common, often with torso or neck movement
- More significant misplaced CVCs include catheter tip floated distally (e.g. from IJ into subclavian towards hand)
- Procedure: Arterial Misplacement
- Artery punctured with introducer needle (but not dilated)
- Artery dilated and catheter placed
- Leave in Place Pending Consultation
- Risk of Hemorrhage on large bore Arterial Line removal
- Consult vascular surgery or Intervention Radiology regarding guidance
- Procedure: Venous Misplacement - Catheter Repositioning or Replacement
- Prevention
- Right sided central veins are preferred (less likely for malposition)
- Guidewire should be inserted with its J-curve directed towards the heart at midline
- Catheter Repositioning
- Increases risk of infection and may be more difficult to redirect
- Perform under same sterile conditions as if placing a new catheter
- Requires determining length the catheter needs to be withdrawn before advancing again
- Thread a guidewire through catheter with its J-Curve directed medially toward heart
- Other measures
- Pull downward on ipsilateral arm
- Consider Balloon tipped 2F Fogarty Catheter (longer than CVC) to help float tip into correct position
- Compress the unintended vessel (e.g. subclavian vein) when attempting to reposition into SVC/atrium
- Catheter Replacement (preferred)
- Risks loss of access, but is preferred for decreased infection risk
- Practice same sterile technique and procedure as per new CVC Placement
- Double glove with 2 sets of sterile gloves
- Remove the first glove set after the old catheter has been removed
- New sterile catheter set reduces risk of infection
- Withdraw first catheter from malpositioned location, but still in vessel
- Thread a guidewire through catheter with its J-Curve directed medially toward heart
- Ideally, use a 60 cm guidewire (instead of a standard 45 cm guidewire)
- Alternatively guidewire from new set may be used to change over the old catheter
- Continue to thread the guidewire to proper distance (<20 cm)
- Ideally, use a 60 cm guidewire (instead of a standard 45 cm guidewire)
- Remove the old catheter
- Thread the new catheter over the guidewire
- Precautions
- Use portable XRay or Bedside Ultrasound to monitor catheter positioning during procedure
- Prevention
- References
- Warrington (2021) Crit Dec Emerg Med 35(4): 9
- Roldan (2015) West J Emerg Med 16(5): 658-64 +PMID: 26587087 [PubMed]
- Complications
- Catheter Site Bleeding
- Apply manual pressure to bleeding site for 20 minutes (e.g. sandbag, compression device)
- Purse Stitch
- Woggle Technique
- https://cairweb.ca/en/news/a-pearl-i-learned-and-remembered-the-woggle-technique/
- https://www.stepwards.com/?page_id=24971
- Technique
- Suture (3-0 Monofilament) placed through skin, under the Central Line (careful not to puncture the line)
- Cut off the needle and pull the ends up, twist ends together and thread through an open stopcock
- Push the stopcock against skin (or against intervening gauze) and tighten the stopcock to cinch
- Leave in place for 30 minutes, release the stopcock and remove the Suture
- Sacchetti in Swadron (2022) EM:Rap 22(8): 8
- Other measures
- Resources
- Internal Jugular Vein cannulation video (ACEP Critical Decisions Video)
- Subclavian vein cannulation from a supraclavicular approach video (ACEP Critical Decisions Video)
- Subclavian vein cannulation from an infraclavicular approach video (ACEP Critical Decisions Video)
- Femoral vein cannulation video (ACEP Critical Decisions Video)
- References
- Killu and Sarani (2016) Fundamental Critical Care Support, p. 93-114
- Jacquet and Hong (2014) Crit Dec Emerg Med 28(5): 15-22
- Rutherford (2025) Anatomy of Central Venous Access, Hospital Procedures Course, attended 9/12/2025
- Swaminathan and Herbert in Majoewsky (2013) EM:Rap 13(9): 6