Fascia Iliaca Block, Iliacus Fascia
- See Also
- Indications
- Regional Anesthesia covering proximal femur (hip and anterior medial thigh) to knee
- Also provides Regional Anesthesia to medial lower leg and ankle
- Femoral Neck Fracture
- Mid-shaft Femur Fracture (also covered by Femoral Nerve Block)
- Background
- Identical Anesthesia to Femoral Nerve Block without risk of contacting the femoral nerve
- Fascia Iliaca Block misses the lateral femoral cutaneous nerve (unless performed above the inguinal ligament)
- Fascia Iliaca Block misses the obturator nerve (Hip Joint)
- PENG Regional Anesthesia is proximal enough to also cover the obturator nerve
- Contraindications
- Coagulopathy (e.g. Warfarin, Rivaroxaban, Clopidogrel)
- Multi-system Trauma
- Compartment Syndrome
- Complications
- See Regional Anesthesia
-
Local Anesthetic Systemic Toxicity (LAST Reaction)
- Bupivicaine is typically used for this injection (Ropivacaine is safer if available)
- Bupivicaine may cause a fatal reaction if given intravascularly
- Do NOT use 0.5% for this injection (use 0.25%)
- Carefully identify landmarks by exam and Ultrasound
- Do not inject without first withdrawing and confirming the needle is not within a vessel
- Keep Intralipid nearby when performing this injection (see LAST Reaction for protocol)
- Bupivicaine is typically used for this injection (Ropivacaine is safer if available)
- Anatomy
- Landmarks
- Iliacus Muscle
- Femoral nerve
- Originates from the L2 to L4 nerve roots
- Travels under the superficial fascia lata and the deeper fascia iliaca
- Accompanies lateral femoral cutaneous nerve and the obturator nerves
- Injection into the space beneath the Iliacus Fascia
- Provides Anesthesia for all branches of the the L2 to L4 nerve roots
-
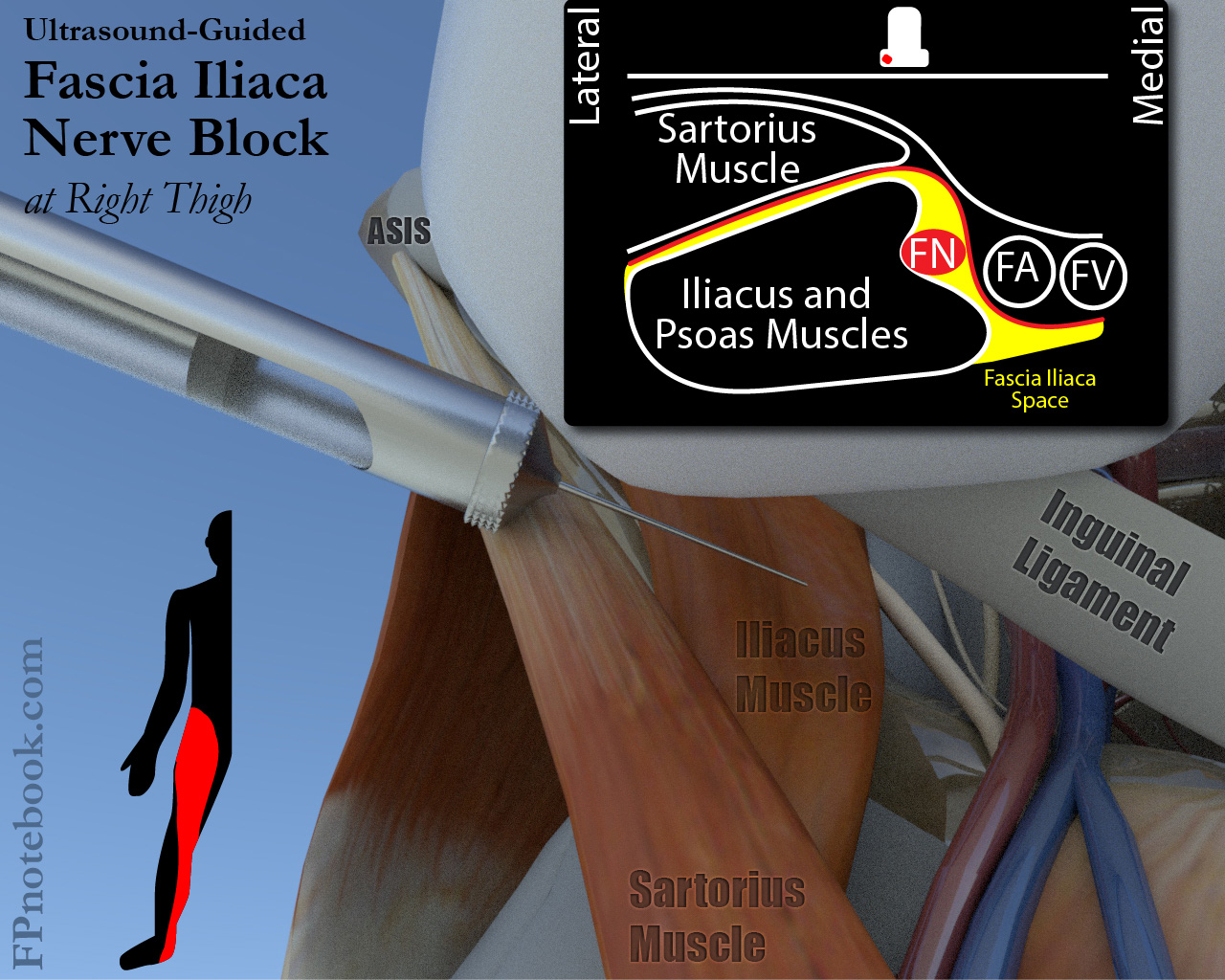
Ultrasound-Guidance (preferred)
- Ultrasound probe positioned parallel to inguinal ligament
- Identify femoral artery and vein in short axis (transverse)
- Femoral nerve will be lateral to femoral artery
- Fascia iliaca will be a bright white line immediately deep to the femoral nerve
- Landmarks
- Inferior to the inguinal ligament
- Superior to the femoral artery bifurcation
- Lateral to the femoral nerve
- Medial to sartorius Muscle
- Slide Ultrasound probe laterally to 2 hyperechoic lines/planes overlying iliacus Muscle
- Pearls
- Direct the needle between the sartorius Muscle and the iliacus Muscle
- Puncture through the fascia iliaca to access the proper injection plane
- Hydrodissection should raise the fascia iliaca up and away from the deeper iliacus Muscle
- Inject well lateral to the femoral nerve
- Avoids nerve injury, and the tissue plane will distribute the Anesthetic
- Injection landmarks (older technique, Ultrasound is preferred instead)
- Divide inguinal ligament into three equal parts
- Mark lateral border of Pubic Symphysis (0 cm)
- Mark at one third (approximately 3 cm)
- Mark at two thirds (approximately 6 cm)
- Mark anterior superior iliac spine or ASIS (approximately 9 cm)
- Injection site should be near the two thirds mark
- Mark approximaly 5-7 cm mark (or 2-4 cm from the lateral margin)
- Confirm position by palpating the femoral artery
- Femoral Artery should be at least 2 fingerbreadths medial to the injection site
- Divide inguinal ligament into three equal parts
- Images
- Preparation
- Patient supine
- Prepare skin (e.g. Chlorhexidine)
-
Local Anesthetic
- Lidocaine 1% for skin and superficial Anesthetic
- Exercise caution with superficial injection, as bubbles will obscure deeper structures on Ultrasound
- Regional Anesthetic
- Dilute Anesthetic to 25-30 cc
- Long-acting Anesthetic options
- Ropivacaine (0.5%): Maximum dose of 2 to 3 mg/kg OR
- Bupivacaine (0.25%): Maximum dose of 2 to 2.5 mg/kg
- Short-acting Anesthetic options
- Lidocaine (1-2%): Maximum dose of 4 mg/kg OR
- Mepivacaine (1.5%): Maximum dose of 4 mg/kg
- Blunt Needles
- 18 gauge blunt needle
- 21 gauge (10 cm, 4 inch) short bevel or Touhy needle with extension set (best visibility on Ultrasound)
- 20 gauge (3.5 inch) spinal needle with extension tubing
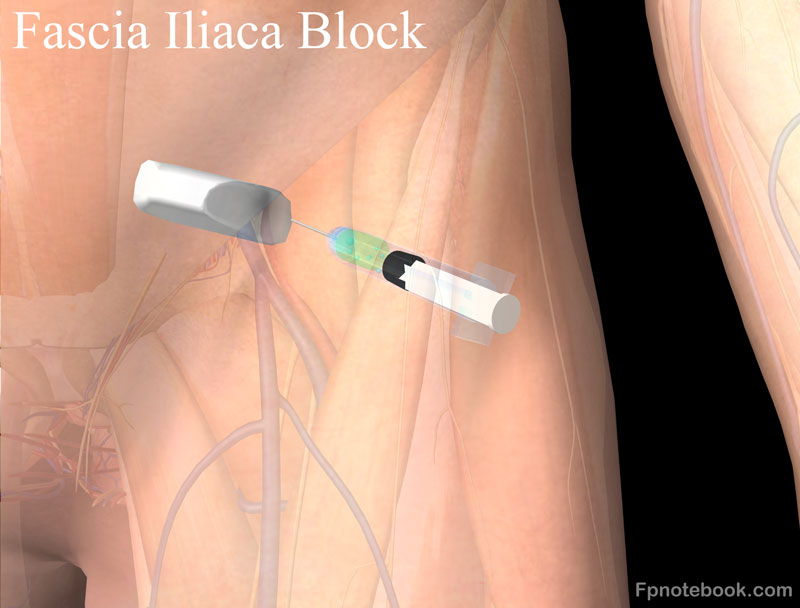
- Technique
- Use Ultrasound-Guidance as above
- Utrasound probe positioned parallel to inguinal ligament
- Raise a skin wheel with the Local Anesthetic over the injection site
- Use an 18 gauge needle to break the skin (do not insert deeply - only make a hole)
- Insert a blunt needle (see options above) through this hole created by 18 gauge needle
- Direct needle, angled lateral to medial in-plane with Ultrasound probe
- Slowly insert needle until a pop is heard or felt as the needle breaches the fascia lata plane
- Slowly insert needle until a second pop is heard or felt when the needle breaches the fascia iliaca
- Ultrasound is preferred for localization (but it is not mandatory)
- Aspirate to confirm not in vessel
-
Ultrasound confirmation of position
- Inject an initial 1 to 2 ml Anesthetic or saline deep to the fascia iliaca can widen the space (hydrodissect)
- Do not inject into Muscle
- Anesthetic will track toward femoral nerve on Ultrasound
- Do NOT inject adjacent to femoral nerve (this is a compartment block)
- Inject the 20-30 cc of diluted Anesthetic
- Injection should flow very easily (as if injecting into an IV)
- Withdraw or advance the needle 1-2 mm if resistance is met
- No swelling should be seen
- Efficacy
- Highly effective and reproducible (even without Ultrasound) as target is
- Will not achieve complete Anesthesia in the leg
- Resources
- References
- Grant and Auyong (2017) Ultrasound Guided Regional Anesthesia, Oxford University Press, New York, 121-5
- Eicken and Rempell (2016) Crit Dec Emerg Med 30(4):3-11
- Herbert and Weingart in Herbert (2019) EM:RAP 19(7): 4, 8-9
- Mason and Capagne in Herbert (2018) EM:Rap 18(9): 2-3
- Sacchetti in Herbert (2012) EM:RAP 12(2): 4