Blood Lactic Acid, Lactic Acidosis, Lactic Acidosis Definition, Lactic Acid
- Physiology
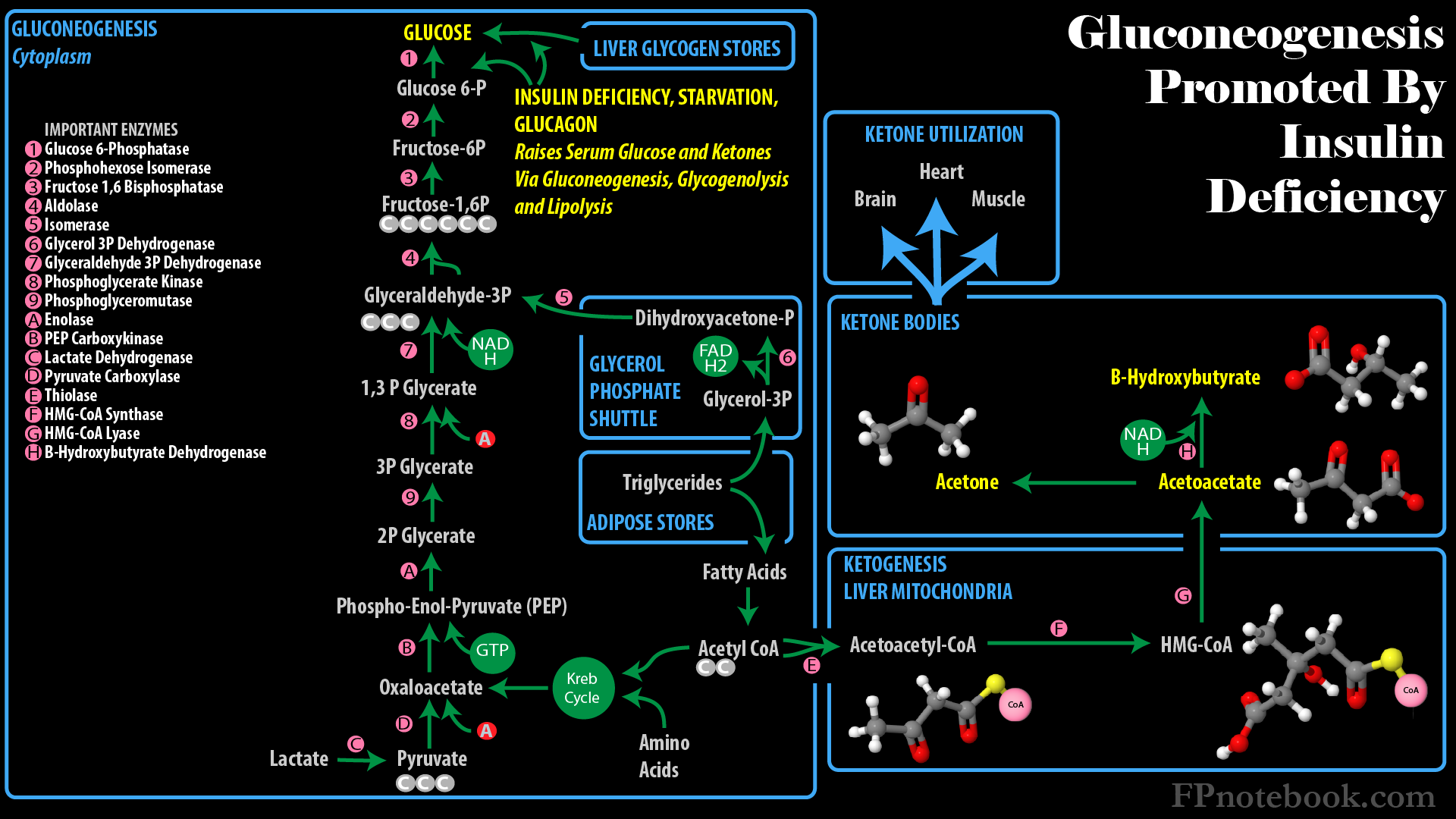
- See Glucose Metabolism
- Lactic Acid is generated when oxygen is unavailable to allow for Krebs Cycle related Oxidative Phosphorylation
- Glycolysis generates 7 net ATP/Glucose (compared with 25 for Kreb Cycle) and does not require oxygen
- However, Glycolysis does use NAD+ (for glyceraldehyde 3-P to 1,3P2-glycerate)

- NAD+ is typically replenished in the Krebs Cycle related Oxidative Phosphorylation
- When oxygen is unavailable, pyruvate is metabolized to Lactic Acid, regenerating NAD+
- Lactic Acid conversion back to Glucose (Gluconeogenesis) requires several additional steps

- Muscle Cells release generated Lactic Acid
- Lactate may be directly utilized by the Heart (up to 60% of energy demands) and brain (up to 25% of energy demands)
- Lactic Acid is transported via systemic circulation to liver and Kidney
- Liver (70-75%) and Kidney (25-30%) cells perform lactate metabolism (Gluconeogenesis)
- Three Enzymes required for Gluconeogenesis from Lactic Acid are only in cells of the liver and Kidney
- Pyruvate carboxylase
- Fructose Diphosphatase
- Glucose 6-Phosphatase

- Causes
- Tissue Hypoxia in Hypoperfusion States (Type A)
- Systemic hypoperfusion or shock
- Hypovolemia or Dehydration
- Cardiogenic Shock
- Seizure (transient)
- Septic Shock
- Lactic Acid is generated in lungs and Muscle, primarily with leukocyte Glycolysis
- Local hypoperfusion
- Testicular Torsion
- Intestinal Volvulus
- Acute Mesenteric Ischemia
- Arterial embolism (e.g. Cerebrovascular Accident)
- Epinephrine infusion (causing tissue Hypoxia)
- Decreased arterial oxygen
- Hypoxemia (e.g. Asthma)
- Severe Anemia
- Carbon Monoxide Poisoning
- Causes
- No Tissue Hypoxia (Type B)
- Medical conditions (Type B1)
- Severe liver disease (related to Cori Cycle Lactic Acid generation)
- Cancer
- Thiamine Deficiency
- Medications or toxins (Type B2, most are via mitochondrial cytopathy)
- Acetaminophen Overdose
- Acetaminophen Poisoning directly inhibits Electron Transport Chain in mitochondria
- Lactic Acidosis in Acute Hepatic Failure is associated with higher mortality
- Cyanide Poisoning
- Cyanide blocks Oxidative Phosphorylation
- Lactic Acid levels are typically very high (>10 mmol/L)
- MetforminOverdose
- Beta-2 Agonist (transient Lactic Acidosis)
- Via stimulated Glycolysis and pyruvate generation
- Albuterol 10 mg neb increases Lactic Acid 0.8 mmoL/L
- Zitek (2016) Acad Emerg Med 23(6): 718-21 +PMID:26857949 [PubMed]
- Isoniazid (via liver toxicity)
- Tetracycline
- Linezolid
- Alcohol and Toxic Alcohol ingestion
- Propofol
- Causes Propofol Infusion Syndrome
- Propylene gylcol (solvent for many Parenteral drugs)
- Nucleoside Reverse Transcriptase Inhibitor (NRTI agents)
- Acetaminophen Overdose
- Congenital metabolic conditions (Type B3)
- Mitochondrial disorders
- Hypoglycemia
- Labs
- Collection
- Draw lactate samples in gray-top tube, cool in ice bag and run sample within 15 minutes
- RBC metabolism will otherwise falsely alter serum lactate levels
- Precautions
- Lactic Acid is primarily used as a Sepsis marker and tissue ischemia marker (e.g. Ischemic Bowel)
- Lactic Acid clearance outside Sepsis does not uniformly improve with Intravenous Fluids
- Cardiogenic Shock can also increase Lactic Acid and will worsen with excess fluids
- Outside Sepsis, Exercise caution in aggressive fluid Resuscitation to lower Lactic Acid
- Lactic Acid is falsely elevated with improper collection
- Delayed Running of a sample (or a sample not kept on ice after blood draw)
- Non-free flowing sample (e.g. Tourniquet in place during blood draw)
- Arterial Line samples are most accurate (free flowing)
- Controversial as to whether Tourniquet use effects lactate level
- Lactic Acidosis is associated with increased mortality in specific conditions (esp. Lactic Acid >4 mmol/L)
- Septic Shock
- Cryptic Shock (occult hypoperfusion) with normal Blood Pressure, but increased Lactic Acid level
- Trauma
- Failure to clear Lactic Acid
- May indicate infectious disease complications, organ dysfunction and inadequate Resuscitation
- Expect Potassium to increase with severe Lactic Acidosis
- Severe Lactic Acidosis (typically >4) is associated with a Metabolic Acidosis with Anion Gap
- Cellular Potassium-hydrogen transporter drives hydrogen into cells in exchange for Potassium
- Potassium efflux from cells results in an increase in Serum Potassium
- References
- Claudius and Kallay in Swadron (2023) EM:Rap 23(5): 9-10
- Herbert and Crager in Herbert (2018) EM:Rap 18(4): 1-3
- Efficacy
- Children
- Lactic Acid has historically not been used in children, as much as it has become a mainstay in adult evaluation
- Lactic Acid may have more evidence for use in sick children (esp. Sepsis, Trauma) and their disposition
- Increased organ dysfunction in children with elevated Lactic Acid >4 mmol/L
- Predicted need for Critical Care in children with Trauma and pre-hospital elevated Lactic Acid >4 mmol/L
- Predicted in-hospital mortality for critically ill children
- References
- Platzer and Ponce (2023) Crit Dec Emerg Med 37(5): 16-7
- (2013) Endo and Acid Base Disorders, EM Bootcamp, Las Vegas