Rotator Cuff Injury, Rotator Cuff Syndrome
- Epidemiology
- Rotator Cuff is responsible for most Shoulder Pain
- Age of onset typically over 40 years old
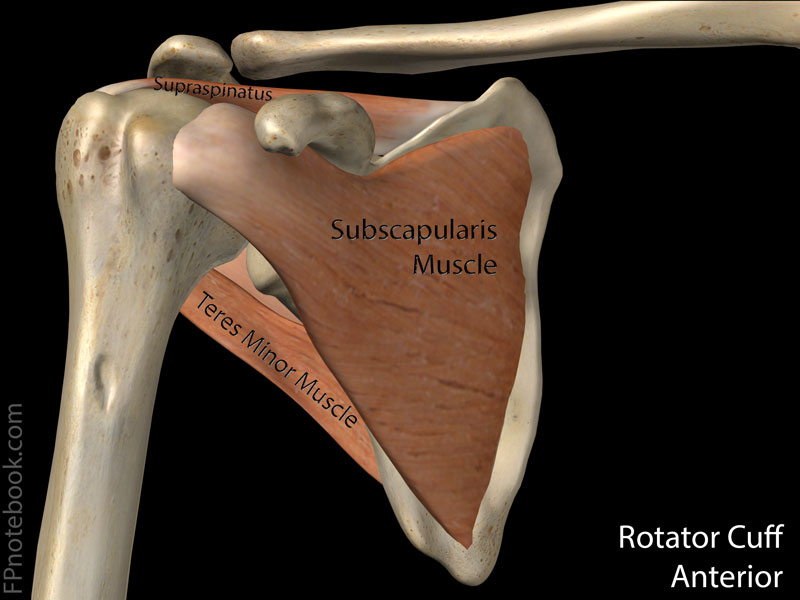
- Anatomy
- See Shoulder Anatomy
- Rotator Cuff fuses near humeral tuberosity
- Image
- Risk Factors
- Predisposition for injury increases with advancing age
- Trauma at tendons (especially supraspinatus)
- Secondary inflammation
- Thickening at subacromial bursa
- Symptoms
- Characteristics
- Lateral arm without radiation beyond elbow
- Associated with arm weakness
- Timing
- Night pain interferes with sleep
- Provocative
- Exacerbated by throwing motion
- Overhead work
- Signs
- Painful arc
- Positive Shoulder Impingement Signs
- Differential Diagnosis
- See Shoulder Pain
- Imaging
-
Shoulder XRay (first-line)
- Calcific Tendonitis
- Hook Acromion (See Acromion XRay Findings)
- Bone cysts or sclerosis within humeral head
-
Shoulder Ultrasound
- Evaluates Rotator Cuff Tears (esp. full thickness) well
- Best in patients older than age 40 years old (tend to have full thickness tears)
- Rotator Cuff is nearly identical appearance as T2w MRI (with an inverse/negative of brightness/echogenicity)
-
Shoulder MRI
- Best at evaluating differential diagnosis (e.g labral tear)
- Best in patients younger than age 40 years (tend to have partial tears and other pathology)
- Management
- Sample Protocol
- See specific Rotator Cuff conditions
- Initial Visit
- Evaluate for serious Traumatic Injury
- Careful Shoulder Exam
- Shoulder XRay
- Start Conservative Therapy
- Evaluate for serious Traumatic Injury
- Next Visit (at 3 weeks from onset)
- Consider Subacromial Corticosteroid Injection for severe or refractory symptoms
- Adjust activity restrictions
- Consider MRI and Orthopedic Consultation if suspect large Rotator Cuff Tear
- Traumatic Injury
- Severe pain and weakness
- Positive Drop Arm Test
- Weakness on Empty Cans Testing (esp. if persists despite injection)
- Next Visit (at 6 to 12 weeks from onset)
- Adjust activity restrictions
- Consider MRI and Orthopedic Consultation
- Suspected partial Rotator Cuff Tear and persistent symptoms
- Next visit (at 6 months from onset)
- Reevaluate Shoulder function and pain
- Consider permanent change in job duties if recurrent reinjury
- Consider repeat Subacromial Corticosteroid Injection
- Consider MRI and referral for persistent symptoms (esp. if Hook Acromion)
- Consider advanced measures (typically by sports medicine)
- Extracorporeal shock wave therapy
- Dextrose prolotherapy
- Platelet-rich plasma injection
- No benefit compared with saline injection Placebo
- Hurley (2019) Arthroscopy 35(5): 1584-91 [PubMed]
- Avoid Unhelpful Measures
- Kinesiology taping is no better than sham therapy in Rotator Cuff disease
- No benefit in overall pain, function, range of motion or quality of life
- Gianola (2021) Cochrane Database Syst Rev (8): CD012720 [PubMed]
- Kinesiology taping is no better than sham therapy in Rotator Cuff disease