Atrioventricular Block, Atrioventricular Node Block, AV Block, AV Node Block, First Degree Atrioventricular Block, Second Degree Atrioventricular Block, Third Degree Atrioventricular Block, Complete Atrioventricular Block, Sinoatrial Exit Block, Wenckebach AV Block, Mobitz I AV Block, Mobitz II AV Block, Heart Block
- Pathophysiology
- Impaired conduction in Atria, AV Node or His-Purkinje
- Types
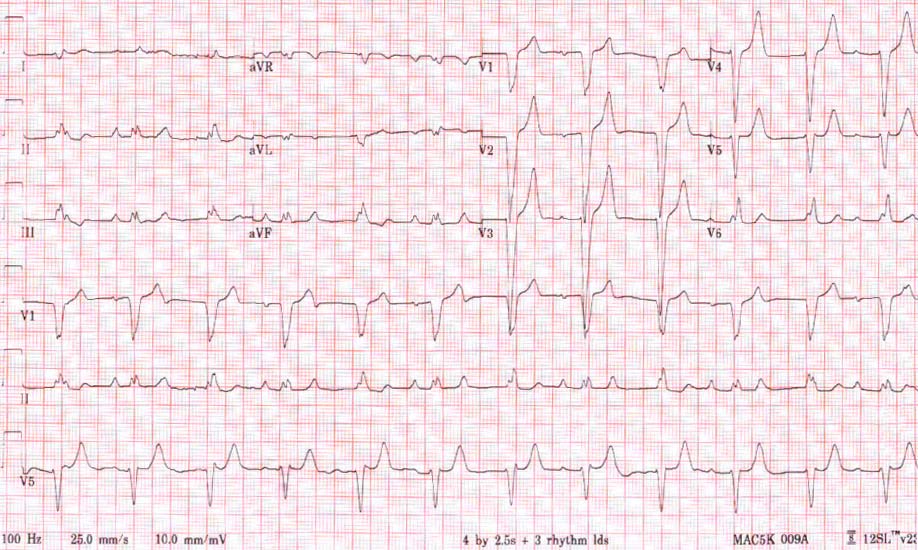
- First Degree Atrioventricular Node Block
- Causes
- Normal finding in >1% of healthy adults
- Inferior wall ischemia (right Coronary Artery) if onset in acute presentations
- Increased vagal tone (responds to Atropine)
- Hypothyroidism
- Medications
- Findings
- Consistently Prolonged PR Interval >0.20 seconds
- Each P Wave is conducted and associated with a QRS Complex
- Treatment
- None needed
- Types
- Second Degree Atrioventricular Node Block
- Also known as Sinoatrial Exit Block
- Type I Second Degree Atrioventricular Node Block
- Known as Mobitz I AV Block or Wenckeback Conduction
- Acute condition affecting AV Node
- Most often due to excess vagal tone
- EKG Findings
- Progressive increase PR Interval until beat/QRS Complex dropped (non-conducted P Wave)
- Cycle repeats after beat dropped, with PR Interval resetting aftet the dropped beat
- Causes: Functional, reversible defects
- Inferior Myocardial Ischemia
- Rheumatic Fever
- Digitalis Toxicity
- Increased vagal tone
- Beta Blocker
- Response to Maneuvers
- Bradycardia improves in response to Atropine and Exercise
- Worsens with carotid massage
- Type II Second Degree Atrioventricular Node Block
- Known as Mobitz II Block
- Chronic condition affects infranodal conduction path
- Intermittent conduction defect with a consistent frequency of non-conducted P Wave
- Described as a ratio (e.g. 3:2) of P Waves to QRS Complexes
- EKG Findings
- Regularly dropped QRS waves at consistent interval is typical
- Other findings
- No change in PR Interval (remains constant unlike Mobitz 1)
- RR interval is constant, except for the missed beat, which is then double the PP interval
- QRS Duration does not differentiate Mobitz 1 from 2 (either may have a normal or prolonged QRS)
- Although typically infranodal, the defect may lie within the AV Node in some cases
- Causes: Structural, non-reversible defects
- Anterior Wall or Anteroseptal Myocardial Infarction (most common cause)
- Infiltrative, fibrotic or sclerotic cardiac conditions
- Lenegre Disease
- Lev Disease
- Cardiomyopathy
- Lymphoma and other cardiac tumors
- Cardiac Amyloidosis
- Collagen Vascular Disease
- Response to Maneuvers
- Prognosis
- Worse than Mobitz I Block
- High risk of progression to complete Heart Block (third degree block)
- Increased risk of Sudden Cardiac Death (if third degree AV Block occurs)
- Indication for cardiac Pacemaker if reversible cause is not identified
- Risk based on EKG Presentation (in increasing order of risk)
- Mobitz II with narrow QRS Complex
- Mobitz II with wide QRS Complex
- Mobitz II with narrow QRS and high grade AV Block
- Mobitz II with wide QRS Complex and high grade AV Block
- Management
- Urgent cardiology Consultation
- Pacemaker indicated
- Types
- Third Degree Atrioventricular Node Block (Complete AV Nodal Block)
- Findings
- Complete electrical and mechanical AV dissociation
- P and QRS waves are present but unrelated
- Images
- Subtypes
- Congenital Third Degree AV Node Block (narrow complex)
- Acquired Third Degree AV Node Block (wide complex)
- Wide complex escape beat at 30 to 45 bpm (infranodal)
- Hemodynamic instability requires stabilization
- References
- Berberian, Brady, Mattu (2024) Crit Dec Emerg Med 38(7): 12-3
- Vandersteenhoven and Brady (2025) Crit Dec Emerg Med 39(2): 13-5