Femoral Neck Stress Fracture
- Pathophysiology
- As with other Stress Fractures, overuse injury more common in female athletes
- Images
- Risk Factors
- See Stress Fracture
- Similar risks to Pubic Ramus Stress Fracture (Military recruits, Distance runners and Dancers age 20 to 30 years old)
- Associated with a sudden increase in Exercise intensity or distance
- Insufficiency Fracture risks
- Relative Energy Deficiency in Sport (RED-S)
- Postmenopause
- Female gender
- Delayed Menarche
- Femoral acetabular impingement
- Low Vitamin D Level
- Smoking
- Metabolic conditions (e.g. Osteoporosis, Hyperparathyroidism, renal disease)
- Symptoms
- Groin Pain or anterior thigh pain, or lateral thigh or buttock pain
- Provoked by activity (weight bearing)
- Relieved with rest (but may cause night pain)
- Signs
- Antalgic Gait
- Provocative maneuvers resulting in pain
- Internal hip rotation
- Weight bearing
- Log Roll Test (Freiberg Test, Passive Supine Hip Rotation)
- Imaging
- Hip XRay
- MRI preferred over nuclear bone scan
- High Test Sensitivity (similar to bone scan)
- High Test Specificity (better than bone scan)
- Management
- Early diagnosis and management is critical to avoid a devastating complete Hip Fracture
- Initiate non-weight bearing and avoidance of lower extremity activity while definitive imaging is pending
- Risk Modification
- See Stress Fracture
- Image the opposite hip if Stress Fracture is found (bilateral Hip Stress Fractures are common)
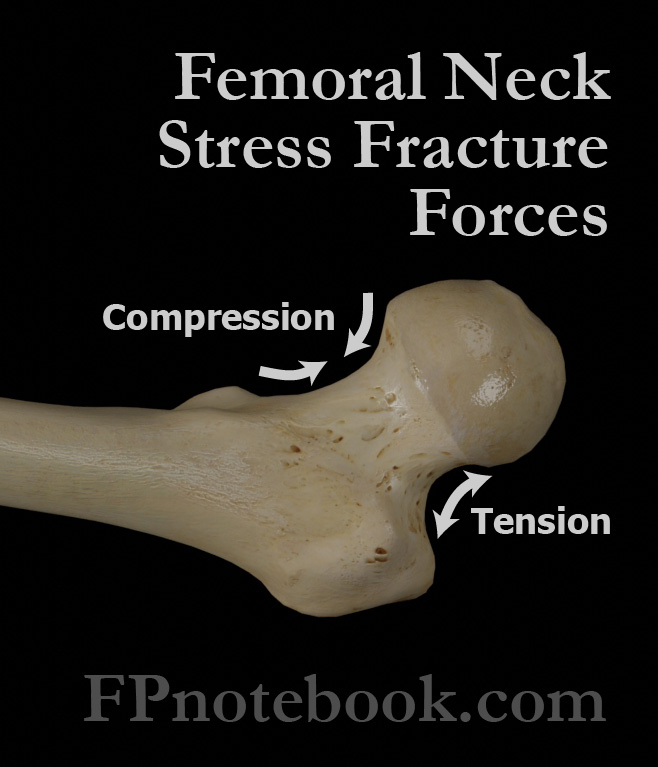
- Inferior Femoral Neck Stress Fractures (medial, compressive or compression side)
- Consult orthopedic surgery
- Period of strict non-weight bearing and crutch use
- Gradual progression to weight bearing activity starts only after pain improves and imaging demonstrates healing
- Typical weight bearing progression occurs over a 4 to 6 week period
- Conservative management (as long as involves <50% of cortex)
- Return to Running and sport in 8-12 weeks
- Superior Femoral Neck Stress Fractures (lateral, tensile or tension side)
- Risk of complete Fracture or Hip Avascular Necrosis
- Consult orthopedic surgery urgently
- Consider percutaneous screw fixation
- Complications
- Complete, displaced Hip Fracture (if not diagnosed early)
- Nonunion Fracture
- Avascular Necrosis
- References
- Shahideh (2013) Crit Dec Emerg Med 27(9):10-18
- Morelli (2001) Am Fam Physician 64(8):1405-1414 [PubMed]
- Schroeder (2022) Am Fam Physician 106(6): 675-83 [PubMed]