Bell's Palsy, Bells Palsy, Bell Palsy, Facial Nerve Paralysis, Facial Nerve Palsy, CN 7 Palsy
- Definitions
- Bell's Palsy (Facial Nerve Palsy)
- Idiopathic, acute Facial Nerve Paralysis
- Background
- History
- Named for Sir Charles Bell (1774-1842) who first described the syndrome
- Epidemiology
- Incidence: 15-30 per 100,000 per year (45,000 per year in U.S.)
- No gender predominance
- Ages most commonly affected 15 to 45 years old (peaks at age 40-49 years)
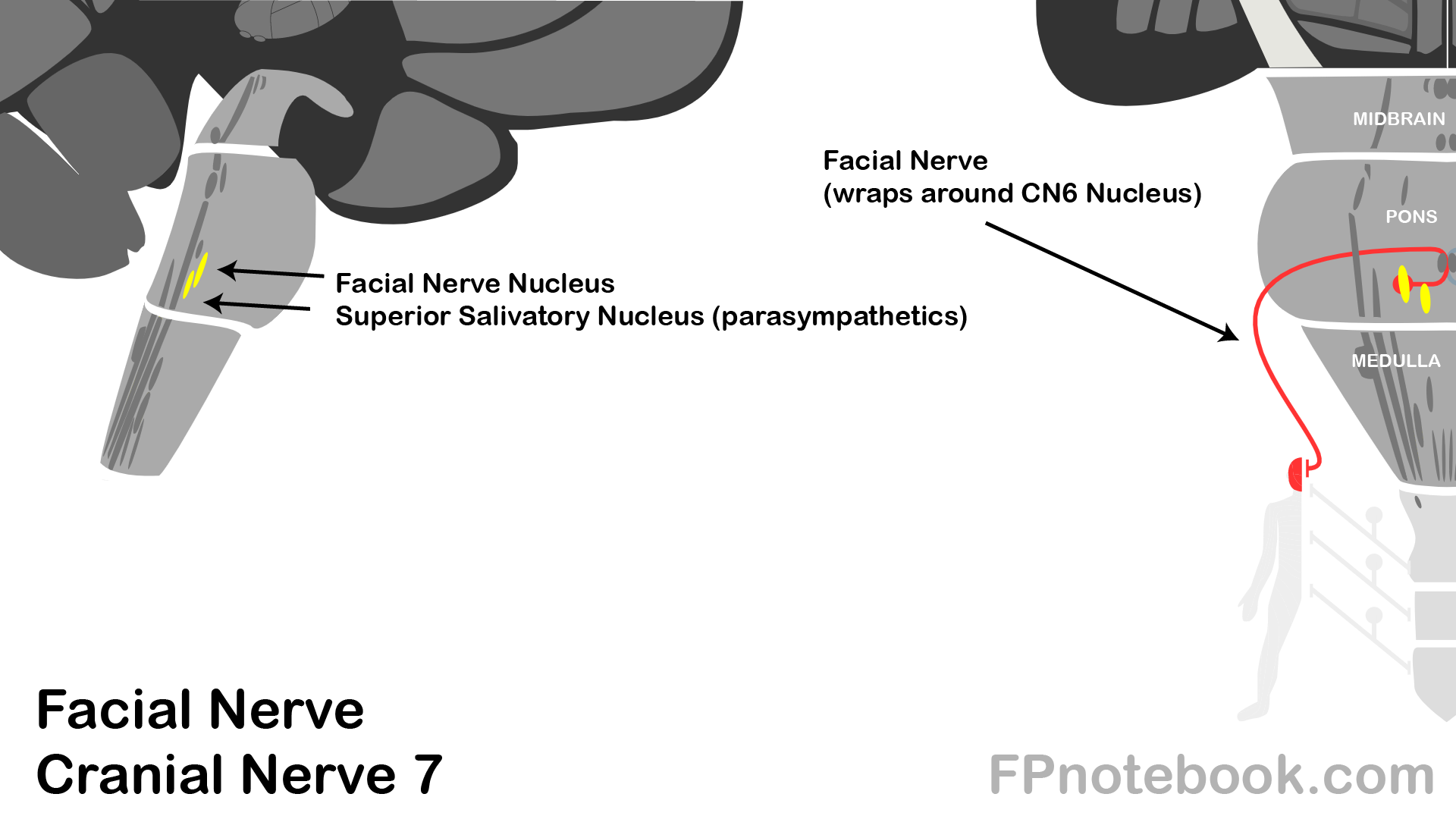
- Pathophysiology
- Bell's Palsy is a Peripheral Nerve disorder (affecting the nerve after exiting its nucleii in the pons)
- Only peripheral CN 7 lesions (Bell's Palsy) affect forehead motor activity
- Both sides of the brain provide input to the forehead (redundant, dual innervation)
- Any lesion affecting forehead motor activity must occur peripherally
- Forehead motor activity (e.g. full Eyelid closure) is preserved in CNS Lesions (stroke)
- Caused by Facial Nerve edema, compression or inflammation
- Typically at Geniculate Ganglion (risk of ischemia, demyelination) after exiting the internal acoustic meatus
- Associated with Herpesvirus infection in 30% of cases
- Images
- Risk Factors
- Diabetes Mellitus (comorbid in 10% of cases)
- Pregnancy (associated with 3 fold increased risk)
- Immunosuppression
- Influenza A
- Herpesvirus infection (comorbid in 30% of cases)
- History
- Red Flags suggestive of other Facial Nerve Paralysis Cause
- Gradual onset over >2 weeks
- Suggests mass lesion
- Mass lesion may also cause a recurrent unilateral Bell's Palsy
- Forehead not involved
- Suggests Central Nervous System cause (supranuclear lesion)
- Facial Nerve motor nucleus is divided
- Dorsal aspect (forehead innervation) and ventral aspect (lower facial innervation)
- Both sides of the brain provide input to the dorsal aspect (forehead)
- Hence lack of forehead involvement implies an Upper Motor Neuron Lesion
- Only one side of the brain provides input to the ventral aspect (lower face)
- Bilateral involvement
- Suggests autoimmune Polyneuropathy
- Lyme Disease
- Recent new medications (e.g. Influenza Vaccine)
- Acute Unilateral Weakness in other distributions (suggests CNS Lesion)
- Extraocular Movement deficits
- Unilateral limb weakness
- Bulbar weakness
- Lyme Disease Risk Factors (Tick Bite, endemic Lyme Disease region during peak season)
-
Fever
- Consider infectious cause such as Otitis Media
- Rash
- Vesicular rash (Herpes Zoster, Ramsay Hunt Syndrome)
- Erythema Migrans (Lyme Disease)
- Hearing Loss and Vestibular Symptoms or Ataxia
- Children (esp. children age <5 years)
- Otitis Media
- Trauma
- Herpes Simplex Virus
- Varicella Zoster Virus
- Lyme Disease
- Malignancy (esp. Leukemia, Lymphoma, Brain Tumor)
- Associated with a 0.7% risk in children age <5 years (contrast with 0.3% overall)
- Evaluate for Hepatosplenomegaly and Lymphadenopathy, and ensure close follow-up
- References
- Claudius and Walsh (2022) EM:Rap 22(9): 8-9
- Walsh (2022) Am J Emerg Med 53:63-7 +PMID:34992025 [PubMed]
- Exam
- Head and neck
- External Ear and ear canal (e.g. Otitis Externa, Herpes Zoster, Ramsay Hunt Syndrome)
- Tympanic Membrane (e.g. Otitis Media)
- Mouth and pharynx (e.g. Herpes Simplex Virus)
- Parotid Gland
-
Neurologic Exam
- Perform complete Neurologic Exam including gait
- Perform extremity Motor Exam and Sensory Exam
- Cranial Nerve Exam
- Test Cranial Nerve 7 bilaterally on lower face and forehead (forehead MUST be involved in Bell's Palsy)
- Raise eyebrows, wrinkling forehead
- Close eyes tightly
- Frown
- Show teeth
- Pucker lips
- Skin
- Vesicular rash (Herpes Zoster, Ramsay Hunt Syndrome)
- Erythema Migrans (Lyme Disease)
- Symptoms
- Idiopathic Facial Nerve Paralysis developing over 1 to 3 days
- Associated symptoms or signs
- Hypoesthesia or dysesthesia (80%)
- Glossopharyngeal Nerve dysfunction
- Trigeminal Nerve dysfunction
- Facial or retroauricular pain (60%)
- Dysgeusia (57%)
- Hyperacusis (30%)
- Vagal nerve motor weakness (20%)
- Decreased Lacrimation (17%)
- Trigeminal Nerve motor weakness (3%)
- Synkinesis (e.g. mouth twitching while blinking, or winking while smiling)
- Hypoesthesia or dysesthesia (80%)
- References
- Signs
- General
- Preserved facial Sensation
- However hypoesthesia or dysesthesia is common (see above)
- Mouth and nasolabial changes
- Loss of facial creases and flattening of nasolabial fold
- Corner of mouth droops
- Eye changes
- No furrow over forehead (forehead appears flattened)
- Critical to recognize when the forehead and Eyelid are not involved
- Lack of forehead and Eyelid involvement suggests an Upper Motor Neuron Lesion such as a CVA
- Signs
- Facial Nerve Grading (House-Brackman)
- Grade 1: Normal Facial Nerve Function
- Grade 2: Mild Facial Nerve Dysfunction
- Gross
- Slight weakness on close examination
- Synkinesis slight
- Rest: Normal symmetry and tone
- Motor Exam
- Forehead: Moderate to good function
- Eyes: Complete closure with minimum effort
- Mouth: Slight asymmetry
- Gross
- Grade 3: Moderate Facial Nerve Dysfunction
- Gross:
- Obvious difference between sides (not disfiguring)
- Synkinesis noticeable
- Rest: Normal symmetry and tone
- Motor Exam
- Forehead: slight to Moderate movement
- Eyes: Complete closure with effort
- Mouth: Slightly weak with maximal effort
- Gross:
- Grade 4: Moderately Severe Facial Nerve Dysfunction
- Gross
- Obvious weakness
- Disfiguring asymmetry
- Rest: Normal symmetry and tone
- Motor Exam
- Forehead: No motor function
- Eyes: Incomplete closure
- Mouth: Asymmetric with maximal effort
- Gross
- Grade 5: Severe Facial Nerve Dysfunction
- Gross: Barely perceptible motion
- Rest: Asymmetry
- Motor Exam
- Forehead: No motor function
- Eyes: Incomplete closure
- Mouth: Slight movement
- Grade 6: Total Facial Nerve Paralysis
- References
- Differential Diagnosis
- Labs
- Labs are not indicated in isolated peripheral Facial Nerve Paralysis
-
Serum Glucose is not routinely recommended
- Diabetes Mellitus does not cause Bell's Palsy, and is simply a predisposing factor
- Lyme Antibody titer is not routinely recommended
- Lyme peripheral facial palsy is almost always associated with other findings (e.g. Arthritis, facial swelling, rash)
- Isolated Facial Nerve Palsy is not typically due to Lyme Disease
- However, consider empiric therapy for Lyme Disease and lyme test with risk factors in endemic regions
- Bilateral Facial Nerve involvement (high risk, treat as Lyme Disease while testing)
- Known recent deer Tick Bite
- Erythema Migrans (diagnostic without Lyme Titer)
- Peak season in endemic Lyme Disease region
- References
- Imaging
- MRI Head With and Without Contrast
- Benefits
- MRI Identifies central causes (Schwannoma, Hemangioma, meningioma and Cholesteatoma)
- MRI offers prognostic information based on nerve contrast enhancement
- Indications
- Suspected central cause (see Red Flags above)
- Persistent or progressive peripheral Facial Nerve Palsy lasting >2 months
- Facial twitching or spasm
- Recurrent Bell Palsy
- Management
- Corticosteroids and Antimicrobials
- Approach
- Start Corticosteroid within 72 hours of onset
- Antiviral may be considered in moderate to severe cases (House-Brackman Grade 4 and above)
- Consider Lyme Disease management if suggested by history or exam
- Doxycycline (preferred) 100 mg bid or Amoxicillin 500 mg tid for 14-21 days
- High dose Corticosteroids: Prednisone or Prednisolone (primary intervention)
- Adult
- Protocol 1: 60 to 80 mg orally daily for 7 days
- Protocol 2: 60 mg daily for 5 days, then taper off over 5 days
- Worse recover was associated with cummulative Prednisone dosing <450 mg
- Child: 2 mg/kg/day (up to adult dosing) for 7 days
- NNT 10 for full recovery in Bell Palsy treated with early Corticosteroids (<72 hours from onset)
- Salinas (2010) Cochrane Database Syst Rev (3):CD001942 +PMID:20238317 [PubMed]
- Adult
-
Antiviral Agents (optional)
- Mechanism
- Based on reactivated HSV hypothesis
- Indications
- Findings consistent with Herpes Zoster, herpes simplex or Ramsay Hunt Syndrome (e.g. vesicular rash)
- Antiviral may be considered in moderate to severe cases (House-Brackman Grade 4 and above)
- Efficacy of empiric Antiviral use (excluding cases of herpetic, vesicular rashes which should be treated)
- Original studies showed synergistic benefit with Antivirals in combination with Corticosteroids
- More recent studies show primary improvement with Corticosteroids
- Only marginal added benefit with Antivirals
- Reasonable to offer Antivirals in moderate to severe cases
- However patients should be counseled on low efficacy of Antivirals
- Original studies showed synergistic benefit with Antivirals in combination with Corticosteroids
- Agents
- Acyclovir
- Adult: 400 mg five times per day for 7 days
- Child (>2 years): 80 mg/kg daily (max: 3200 mg/day) divided every 6 hours for 5 days
- Valacyclovir
- Age >12 years: 1 gram orally three times daily for 7 days
- Acyclovir
- References
- Mechanism
- Other antimcrobial considerations
- Consider empiric Doxycycline in Lyme Disease endemic regions (esp. bilateral, peak tick season, known Tick Bite)
- Management
- Loss of Blink Reflex
- Rewetting the eye
- Frequent use of preservative-free artificial tears (every 15 to 30 minutes)
- Refresh PM ointment six times daily
- Protective glasses with side pieces
- Use in outdoors, drafty, dusty areas
- Alternatively can use eye shield or cup
- Avoid grinding, sanding, or sawing
- At night:
- Apply bland ointment (Refresh PM, Lacri-Lube)
- Tape eye shut
- Ophthalmology Consultation indicated for incomplete Eyelid closure persisting for weeks
- Risk of Keratitis, Corneal Ulcers and permanent ocular injury from dry, unprotected eye
- Management
- Associated Conditions
-
Otitis Media or Mastoiditis Complications
- IV Antibiotics
- Otolaryngology Consultation for possible wide incision of Tympanic Membrane
-
Herpes Zoster Oticus (Ramsay Hunt Syndrome)
- See Herpes Zoster for Antiviral Agents
- May be associated with Tinnitus and Hearing Loss
- High dose Corticosteroids (1 mg/kg/day)
- Avoid in Diabetes Mellitus, Peptic Ulcer, Glaucoma
- Management
- Referral Indications
- Otitis Media complications
- Mastoiditis complications
- Signs of secondary cause
- Intracranial lesion or nerve impingement
- Incomplete Eyelid closure persisting for weeks
- Risk of permanent ocular injury from drying
- Referral to ophthalmology for management beyond artificial tears
- Other procedure referrals NOT routinely recommended
- Facial Nerve decompression surgery (may rarely be indicated)
- Laser Therapy
- Hyperbaric oxygen
- Intratympanic Corticosteroid Injection
- Stellate Ganglion block
- Physical Therapy (no evidence of benefit in Bell's Palsy)
- May consider for >3 month of Grade 5-6 findings
- Prognosis
- Factors associated with poor prognosis
- Worse Prognosis with time needed for recovery
- No recovery by 3 weeks suggests worse prognosis (15% of cases)
- Further recovery occurs over 3-5 months
- Hyperacusis
- Diabetes Mellitus
- Hypertension
- Pregnancy
- Facial Nerve with severe degeneration by EMG
- Decreased tearing
- Age over 60 years
- Ramsay Hunt Syndrome (Herpes ZosterVirus)
- Severe pain
- Aural pain
- Anterior facial pain
- Radicular pain
- Complications
- Corneal Ulceration or Keratitis (due to incomplete Eyelid closure)
- Permanent Eyelid weakness
- Permanent facial asymmetry (e.g. impaired smiling)
- May be trigger social anxiety, depressed mood and other related complications
- Synkinesis (up to 26% of patients at one year from onset)
- Misdirected nerve regrowth leads to co-contraction of unrelated Muscles innervated by CN7
- Example: Blinking make occur with smiling
- Prognosis
- Early full recovery (66 to 85%) within 3 weeks (higher rates after 8 weeks)
- Children age <14 years and pregnant women have full recovery in 90% of cases
- Prolonged recovery (15%) over 3-5 months (higher risk with bilateral or severe Bell's Palsy)
- Slight residual deficit: 12%
- Mild residual deficit: 13%
- Severe residual deficit: 4%
- Facial weakness
- Contracture or spasm
- Recurrence: 6.5 to 8% of cases (mean interval 10 years)
- Higher risk of recurrence in Diabetes Mellitus
- Complete recovery in 66% of recurrent cases
- Course
- Maximal weakness at 3-7 days after onset
- Most cases (85%) improve within 3 weeks even without treatment
- Additional improvement may require up to 5 months
- Prolonged recovery duration required for nerve regeneration
- References
- Herbert et al in Herbert (2015) EM:Rap 15(11): 3-4
- Zalvan (1999) Consultant 39(1):39-48
- Zvonar and Welsh (2021) Crit Dec Emerg Med 35(2): 25
- Albers (2014) Am Fam Physician 89(3): 209-12 [PubMed]
- Dalrymple (2023) Am Fam Physician 107(4): 415-20 [PubMed]
- Gilden (2004) N Engl J Med 351:1323-31 [PubMed]
- Holland (2004) BMJ 329:553-7 [PubMed]
- Tiemstra (2007) Am Fam Physician 76:997-1002 [PubMed]