Complement Pathway, Complement C3, Complement C4, Complement CH50, Complement Activation, Alternative Complement Pathway, Classical Complement Pathway, Mannose-Binding Lectin Complement Pathway, Complement Disorder, Complement Deficiency Disease, Complement Abnormality
- See Also
- Physiology
- General
- Complement is a group of ~15 Proteins (esp. enzyme precursors)
- Hepatic production and secreted into serum
- Contribute to immune response when activated
- Complement are components of both Innate Immunity and the humoral Immune System
- Multiple triggers including Antigen-Antibody complex as well as direct exposure to pathogen (see activation below)
- Results in inflammatory response (Chemoattractant), Phagocytosis (as Opsonin on cell surface) and pathogen lysis
- Other complement functions
- Solubilizes immune complexes to aid in clearance
- Attaches Antibody-Antigen complexes to Red Blood Cells for transport to the Spleen and liver
- Promotes Bacterial Agglutination
- Neutralization of viral pathogens
- In some cases, inhibits Antigen-Antibody complex formation (and deposition)
- Physiology
- Complement Pathway
- Images
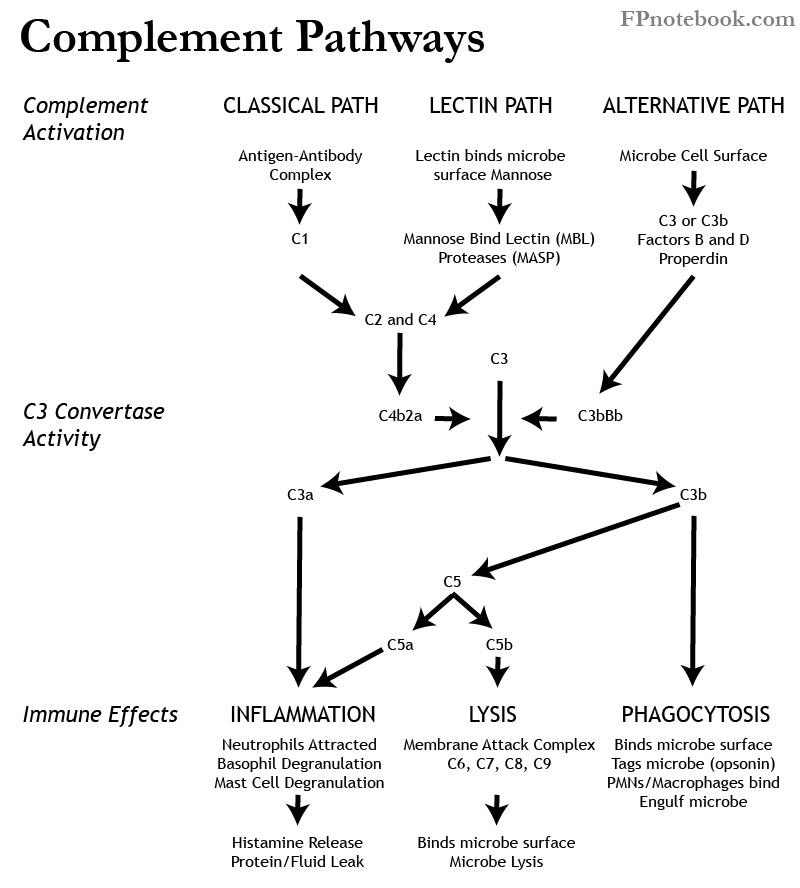
- Activation
- Classical Pathway (C1, C2, C3, C4)
- Alternate Pathway (Properdin, Factor B, Factor D, C3)
- Lectin Pathway (Mannose Binding Lectin or MBL)
- Mannose Binding Lectin (MBL) binds mannose on Microbe surface
- Mannose Binding Lectin Associated Proteases (MASP-1, MASP-2) are activated
- Classical Pathway (above) is stimulated
- Enzyme C3 Convertase (C3bBb or C4b2a) Formation
- Enzyme C3 Convertase splits C3 into C3a and C3b
- C3a stimulates inflammation (attracts Neutrophils, Histamine release from Mast Cells and Basophils)
- C3b results in Opsonization, and stimulates Phagocytosis, and lysis (see below), as well as inflammation (as with C3)
-
Opsonization
- Microbe coated with an Opsonin such as an Antibody or complement (e.g. C3b)
- Surface Opsonins target Microbes for Phagocytosis by Neutrophils and Macrophages
-
Phagocytosis
- Phagocytes such as Neutrophils (PMNs) and Macrophages attract and engulf targeted organisms
- Inflammation (via C3a, C5a)
- Lysis
- Labs
- Complement C3
- Marker for Intrinsic and Extrinsic Pathway Function
- Measured by immunochemical assay
- Complement C4
- Marker for Intrinsic Pathway Function
- Measured by immunochemical assay
- Deficient in 1% of population
- Deficient in 11% with Systemic Lupus Erythematosus
- Complement CH50
- Marker for function of entire intrinsic cascade
- Measured by serum ability to lyse IgG coated RBCs
- Most affected by delay in performing assay
- Causes
- Low Complement levels indicate depletion
- Rheumatic causes
- Systemic Lupus Erythematosus
- Mixed Connective Tissue Disease (MCTD)
- Vasculitis (especially cryoglobulinemia)
- Non-Rheumatic Causes
- Septic Shock
- Liver failure
- Severe Malnutrition
- Pancreatitis
- Severe burns
- Atheromatous embolization
- Indications
- Follow rheumatic disease activity
- Complement fall 20% below baseline signal exacerbation
- Associated Conditions
- Complement Disorders (2% of Immunodeficiency disorders)
- Autoimmune Condition or Rheumatologic Condition (associated with C1-C4 deficiencies)
- Recurrent encapsulated organism, esp. pyogenic infections (manifestations vary depending on missing complement type)
- Complement deficiencies include C1q, C2-C9 (except C4), Factor I, Properdin
- Neisseria infections are most common including Meningitis, Sepsis and Arthritis (associated with C5-C9 deficiencies)
- Recurrent infections with Streptococcus Pneumoniae and Haemophilus Influenzae (associated with C3 deficiency)
- Hereditary Angioedema
- References
- Guyton and Hall (2006) Medical Physiology, p. 419-50
- Mahmoudi (2014) Immunology Made Ridiculously Simple, MedMaster, Miami, FL