Insulin, Insulins, Novolin, Humulin, Insulin-Related Errors, Insulin Pen, Insulin Lente, Ultralente Insulin, Humulin 70/30, Novolin 70/30, Novolog Mix 70/30, Humalog Mix 75/25, Ryzodeg 70/30, Insulin Analog
- See Also
- Definitions
- Insulin
- Insulin is a polypeptide produced by pancreatic beta cells, with release stimulated by Blood Glucose concentration
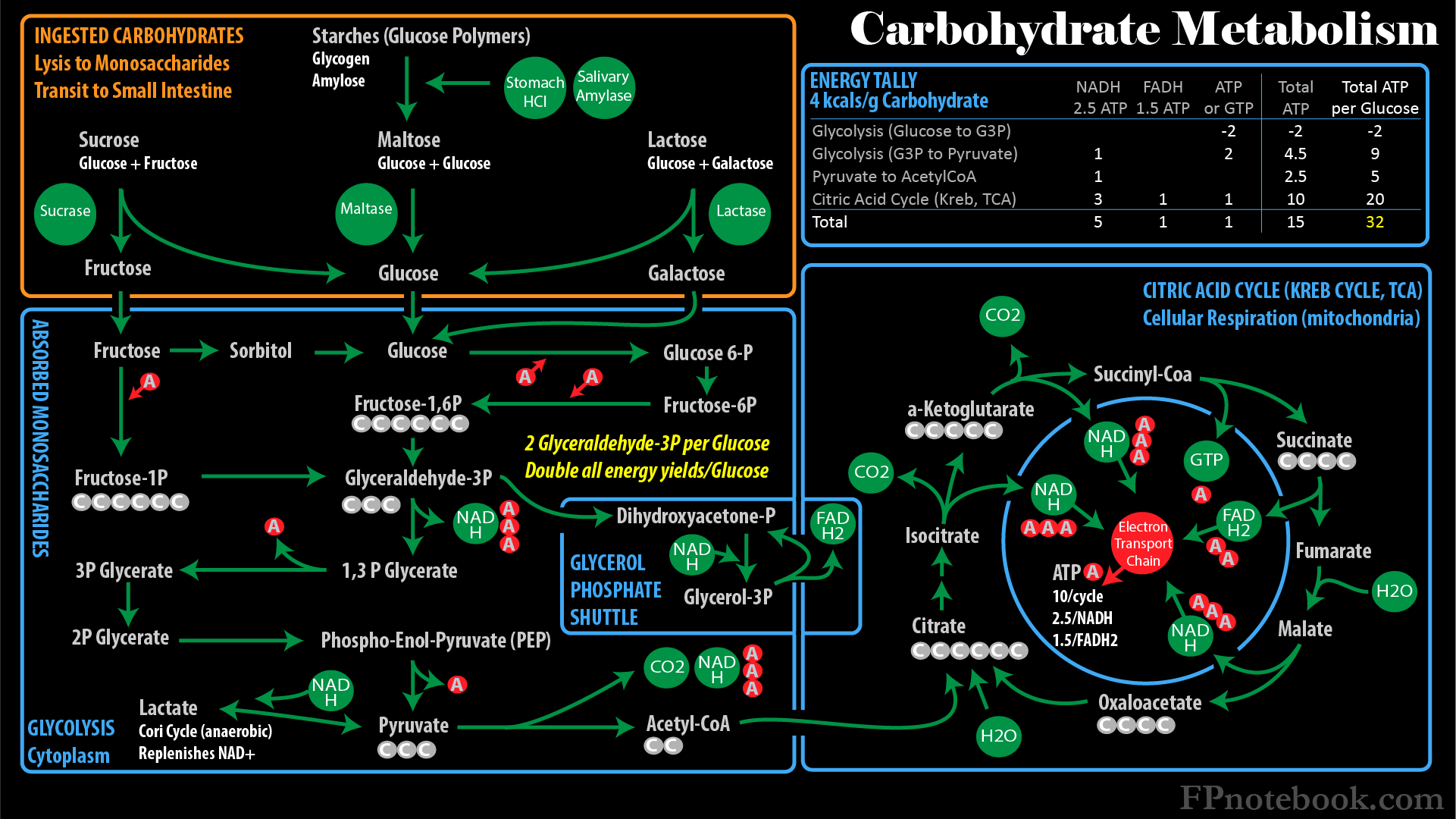
- Insulin promotes energy utilization via Glycolysis, and energy storage as glycogen, Protein and Triglycerides
- First used in Diabetes Mellitus in 1922, by Drs Banting and Best
-
Bolus Insulin (short-acting)
- Similar to physiologic Insulin, with immediate onset (15-30 min) and short duration (2 to 4 hours)
- Primarily covers short-term Blood Glucose spikes with meals
-
Basal insulin (long-acting)
- Long-acting coverage to maintain Blood Glucose control throughout the day, between meals
- Mimics the low level continuous Insulin release by a normal human Pancreas
- Insulin Glargine (Lantus) and similar agents that last approximately 24 hours have largely replaced NPH Insulin (12 hour duration)
- Insulin Analog
- Historically, short-acting Regular Insulin has been sourced from animal Pancreas (pigs, cows)
- As of the 1980s, human Insulins were synthesized in Bacteria
- Synthetic Insulins have since been modfied for rapid onset bolus (e.g. Lispro) and longer-acting basal (e.g. Glargine)
- Physiology
- Images
-
Blood Glucose
- Released from hepatic stores between meals
- Derived from ingested Carbohydrates
- Postprandial Glucose >20 fold over hepatic release
- Insulin
- General
- Insulin is a polypeptide produced by pancreatic beta cells
- Insulin release stimulated by increased Blood Glucose concentration
- Insulin release is also stimulated by glucogenic Amino Acids (all Amino Acids except Leucine and Lysine)
- Insulin response to Glucose is linear
- Overall Insulin effects
- Promotes Glucose uptake by liver and Muscle and for storage as glycogen
- Promotes cellular uptake of Amino Acids and Protein synthesis
- Promotes hepatic synthesis of Fatty Acids, VLDL transport to adipose for Triglyceride storage
- Promotes Glycolysis for energy utilization
- Suppresses Gluconeogenesis
- Muscle Effects
- Increased synthesis of Glycogen, Protein and Triglycerides
- Increased Glucose transport into Muscle Cells
- Hepatic Effects
- Increased synthesis of Glycogen and Protein
- Increased Glucose transport into Muscle Cells
- Increased Glucose utilization for energy (Glycolysis, TCA Cycle)
- Fatty tissue Effects (Adipose)
- Increased synthesis of Glycogen and Triglycerides
- Increased Glucose transport into Muscle Cells
- Phase 1 Insulin Release
- Duration: 10 minutes
- Suppresses hepatic Glucose release
- Phase 2 Insulin Release
- Duration: 2 hours
- Controls mealtime Carbohydrates
- Basal insulin Release
- Low continuous Insulin level
- Covers metabolic needs between meals
- General

- Pathophysiology
- Insulin excess
- See Hypoglcemia
- See Insulin Shock (Insulin Overdose, Insulin Reaction)
- Insulin at low levels or deficiency
- Causes
- Low Insulin due to Diabetes Mellitus
- In Type I Diabetes, Insulin deficiency is key
- In Type II Diabetes, Insulin Resistance is key initially, but later Insulin deficiency results
- Low Insulin as a normal physiologic response to Hypoglycemia
- Low Insulin due to Diabetes Mellitus
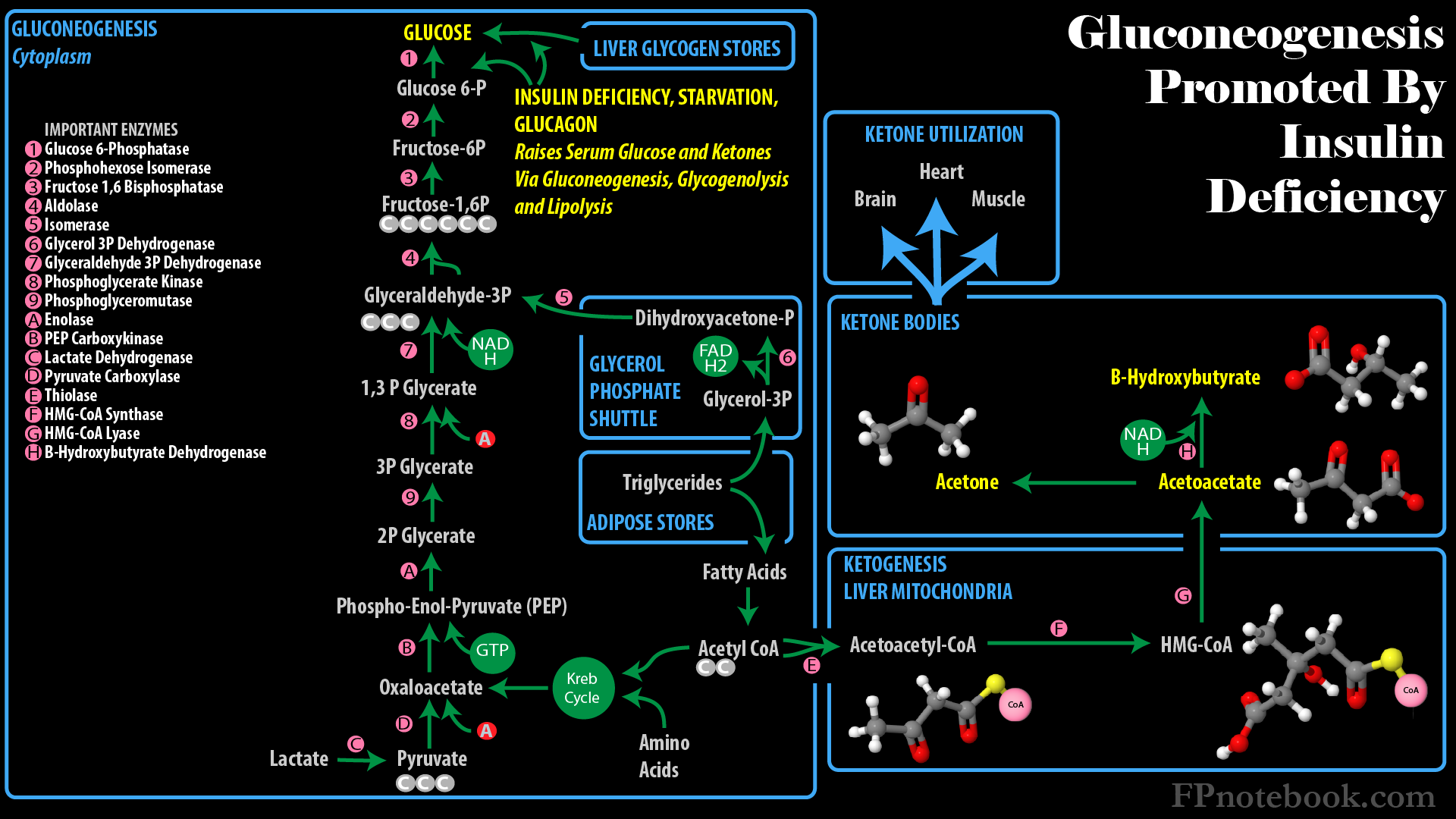
- Low Insulin effects
- Gluconeogenesis and Glycogenolysis results in Hyperglycemia
- Lipolysis (Triglyceride breakdown to Fatty Acids)
- Further lysed into acetyl coA to be utilized in the Kreb Cycle (TCA Cycle, Citric Acid Cycle)
- Other Fatty Acids are diverted to Ketogenesis (Ketone formation)
- Fatty Acids also form excess Cholesterol, Triglycerides within VLDL with increasing atherosclerosis
- Causes
- Technique
- Injection
- Injection sites: Abdomen, outer thigh, back of arm, flank and buttocks
- Insert needle at 90 degree angle into skin
- Insulin injection is subcutaneous (not intramuscular)
- Intramuscular Injection results in rapid absorption and risk of Hypoglycemia
- Prevent too deep of injection (esp. longer needles) by pinching an inch of skin at the injection site
- Hold needle in place for 5-10 seconds after injection to prevent leakage of Insulin
- Rotate injection sites to prevent lipohypertrophy (see adverse effects below)
- Medications
- Insulin Selection
- Insulin anologs are preferred
- More consistent absorption than traditional Insulin
- Bolus analogues have more rapid onset
- Basal agents release at more constant rate
- Insulin anologs are however 10 fold more expensive than Regular Insulin and NPH
- Very high cost results in patients stopping Insulin, resulting in hospitalization and even death
- Vials of NPH Insulin and Regular Insulin are each $26 per vial OTC at Walmart as of 2017
- Contrast with $250 per vial for analogues (e.g. Insulin Lispro, Insulin Glargine)
- Outcomes are similar with newer analogues versus older NPH Insulin and Regular Insulin
- (2015) Presc Lett 22(11):61-2
- (2019) Presc Lett 26(8): 43-4
- Combination agents are discouraged unless noncompliant
- Insulin 70/30 is also $26 OTC at Walmart as of 2017 (Reli-On)
- Reduces flexibility in meal and activity timing
- Medications
- Syringes and needles
- Needle length
- Longer needles risk deeper, intramuscular penetration, with more rapid absorption and Hypoglycemia risk
- Insulin Pen needles 4 mm are sufficiently long
- Insulin syringe needles should be at least 6 mm long to clear the syringe stopper
- Needle gauge
- Smaller needles (higher gauge) 30 or 31 are preferred for the least discomfort on insertion
- Syringe volume
- Select smallest Insulin syringe that will hold each of the Insulin doses, allowing for added coverage
- Prescribe syringes in number of boxes (100 syringes per box)
- Syringes are sized at 100 units Insulin/ml
- Insulin 30 units per 0.3 ml syringe
- Insulin 50 units per 0.5 ml syringe
- Insulin100 units per 1 ml syringe
- References
- (2014) Presc Lett 22(1): 4
- Medications
- Insulin Pens
- Supplied
- Insulin Pens are supplied in boxes of 5 pens each containing 3 ml at 100 units Insulin per ml
- Precautions
- Insulin Pens appear similar to one another despite containing different Insulins (basal or bolus)
- Read each syringe carefully (and note its color) prior to each injection to prevent Overdose errors
- Prepare cloudy Insulins (e.g. NPH) by gently rolling and inverting the pen 10 times prior to injection
- Confirm proper use by asking the patient to demonstrate preparation and injection at clinic visits
- Multidose prefilled pens are intended for use by one individual patient only (do not share pens)
- Sharing pens among patients risks blood borne infection transmission
- Technique
- Attach a new needle to Insulin Pen before each use
- Prime the new needle with 2 units prior to use (removes air bubbles)
- Dial the dose
- Apply to pen to injection site, press the button, and hold in place for 5-10 seconds
- Discard the used needle
- Medications
- Intravenous Regular Insulin
- Note that all other Insulins listed on this page are subcutaneous
- See Insulin Drip
- Onset: Immediate
- Half-Life: 5-10 minutes
- Precautions
- Insulin-Related Errors
- Insulin errors result in >100,000 emergency visits (typically Hypoglycemia related) annually in United States
- Wrong Insulin (Bolus Insulin mistakenly taken)
- Prescribers should carefully check prescriptions and home instructions for errors
- Patients should check Insulin label everytime they inject
- Bolus Insulin in vials and pen devices may be easily mistaken for Basal insulin devices
- Wrong time
- Patients must eat following Bolus Insulin (e.g. Lispro) or do not take Bolus Insulin if plan to skip the meal
- Wrong dose
- Decrease Insulin for anticipated decreased oral intake
- Assist patients with poor Vision or dexterity who have difficulty drawing the correct dose
- Consider syring magnifier, pen device which click per unit, count-a-dose syringe
- Wrong technique
- Mix Insulin suspensions before use (e.g. NPH Insulin, Premixed Insulin such as Insulin 70/30)
- Roll vials or pens 10 times to mix
- Clinic staff should periodically observe patient's technique
- Obtaining fingerstick Glucose
- Calculating their Insulin dose with expected oral intake
- Drawing up Insulin dose
- Injecting Insulin
- Mix Insulin suspensions before use (e.g. NPH Insulin, Premixed Insulin such as Insulin 70/30)
- References
- (2014) Presc Lett 21(7): 40
- Drug Interactions
- Diabetes Agents
- Agents safe to use with Insulin
- Agents safe to use with Basal insulin (Lantus, Levemir); avoid or use caution if used with Bolus Insulin (Lispro, Aspart)
- Sulfonylureas
- Glitinides
- Medications
- Bolus Insulins (Meal-time Insulin)
- See Bolus Insulin
- Traditional Bolus Insulins
- Regular Insulin (Novolin R, Humulin R)
- Onset: 15 to 30 minutes
- Peak: 2.5 to 5 hours
- Duration: 6 to 8 hours
- Avoid in Stage IV or Stage V significant Chronic Kidney Disease
- Avoid if history of severe Hypoglycemia
- Available concentrations
- Humulin R U-100 (100 units/ml, orange)
- Humulin R U-500 (500 units/ml, green)
- High concentration AND basal and Bolus Insulin activity (similar to 70/30)
- See Basal insulins below for description
- Regular Insulin (Novolin R, Humulin R)
- Analogue Bolus Insulins (Rapid, consistent absorption)
- Glulisine (Apidra)
- Onset: 5 to 15 minutes
- Peak: 1 to 2 hours
- Duration: 3 to 5 hours
- Similar to other bolus analogues
- FDA approved to take after meal
- Other analogues expected with same effect
- Lispro (Humalog, Admelog)
- Lispro-aabc (Lyumjev)
- Same manufacturer as Humalog
- Four letter designation refers to new FDA labeling of Insulins as biologics
- Marketed as 10 minutes faster onset that typical Lispro Insulin
- Unlikely to offer any real benefit over other Lispro Insulin
- Concentrations
- Aspart (Novolog, Fiasp)
- Onset: 5 to 15 minutes
- Peak: 1 to 2 hours
- Duration: 3 to 5 hours
- Glulisine (Apidra)
- Medications
- Basal insulins
- Traditional Insulins
- NPH Insulin, Novolin N, Humulin N, Humulin L (Lente)
- Onset: 1 to 2 hours
- Peak: 6 to 8 hours
- Peak time is higher risk of hypoglcemia
- Consider snack at 6 hours after dose
- Duration: 10 to 16 hours (Lente slightly longer)
- Humulin L (Lente) discontinued in U.S. in 2006
- Increased risk of Hypoglycemia (esp nocturnal) compared with newer analogues
- NPH is much less expensive than analogues (still $25/vial as of 2016 at Walmart)
- Humulin R U-500 (500 units/ml, green)
- Indicated for those with very high Insulin requirements (>200 units per day)
- High risk for dosing errors (very concentrated Insulin)
- Specific U-500 green capped syringes are available as of 2016 to reduce dosing errors
- Pens are preferred for less dosing errors over vials and syringes
- Use pen dosing window (not the number of clicks to determine dose)
- Each click of a U-500 pen adds 5 units of Insulin (contrast with 1 unit/click with U-100)
- Activity is similar to Insulin 70/30
- Onset in 30 minutes
- Longer duration (>12 hours) than other Bolus Insulins
- Divide dosing twice (60 and 40%) to three times (e.g. 40, 30 and 30%) daily
- Do not combine with other Insulins (i.e. stop basal and mealtime Bolus Insulins)
- References
- (2022) Presc Lett 29(3): 14
- Ultralente Insulin (extended Insulin zinc suspension)
- Discontinued in U.S. in 2006
- Significant inconsistent effect even in same person
- Onset: 6-10 hours
- Peak: No peak
- Duration: 18 to 24 hours
- NPH Insulin, Novolin N, Humulin N, Humulin L (Lente)
-
Analog Basal Insulin
- See Analog Basal Insulin
-
Insulin Glargine U-100 (Lantus, Basaglar, Semglee)
- Onset: 1-2 hours
- Duration: 21 to 24 hours
- Peak: No peak (flat action curve mimics continuous Insulin Infusion)
-
Detemir U-100 (Levemir)
- Onset: 2-4 hours
- Peak: 6-8 hours
- Duration: 12 to 20 hours (varies by dosage)
- Manufacturer discontinuing drug in U.S. in 2024 (for business reasons)
-
Insulin Degludec (Tresiba)
- Onset: 90 minutes
- No peak activity
- Duration: Up to 42 hours (ultra-long)
- Available as U-100 or U-200
-
Insulin Glargine U-300 (Toujeo, Toujeo Max Solostar)
- Onset: 6 hours
- No peak activity
- Duration: 24 to 36 hours
- Medications
- Combination Agents (Type II Diabetes if poor compliance)
- NPH 70/Regular 30 (Humulin 70/30 or Novolin 70/30)
- Onset: 30 to 60 min
- Peak: 2 to 10 hours (biphasic)
- Duration: 10 to 16 hours
- Aspart Protamine 70/Aspart 30 (Novolog Mix 70/30)
- Onset: 15 min
- Peak: 1 to 4 hours (biphasic)
- Duration: 10 to 16 hours
- Lispro Protamine 75/Lispro 25 (Humalog Mix 75/25)
- Onset: 15 min
- Peak: 1 to 3 hours (biphasic)
- Duration: 10 to 16 hours
- Degludec 70/Aspart 30 (Ryzodeg 70/30)
- Onset: 15 min
- Peak: 2 to 3 hours
- Duration: 24 hours
- Adverse Effects
-
Hypoglycemia
- Increased risk when Hemoglobin A1C <7.4%
- Decreased risk with analogue Insulins
- Higher risk with severe Renal Insufficiency
- Insulin is excreted by the Kidney (30% of total)
- Gluconeogenesis occurs in the Kidney (30% of total)
- Weight gain (Excess of 4 kg over 10 years)
- Lipohypertrophy
- Localized fat hypertrophy and scar tissue from repeated injections in the same area
- Results in variable Insulin absorption as below
- Prevent by rotating injection sites (see below)
- Medical providers should examine injection sites
- Variable Insulin absorption
- Insulin absorption varies by body site
- Variable absorption at lipohypertrophy sites
- Poor absorption causes early postprandial Hyperglycemia
- Depot formation causes delayed Hypoglycemia
- Site rotation (prevents lipohypertrophy - see above)
- Rotate injections within same body region
- Avoids Insulin absorption variability
- Rotate to widely different sites within region
- Example: Abdomen rotate to LUQ, RUQ, LLQ, RLQ
- Rotate injections within same body region
- Reources
- FDA Insulin storage and emergency switching
- References
- (2014) Presc Lett 21(12): 69
- Lepore (2000) Diabetes 49:2142-8 [PubMed]
- Mayfield (2004) Am Fam Physician 70(3):489-512 [PubMed]