Fifth Metatarsal Fracture, Proximal Fifth Metatarsal Fracture, Jones Fracture, Fifth Metatarsal Base Fracture, Fifth Metatarsal Shaft Fracture
- Pathophysiology
- Fifth Metatarsal has thinnest cortical thickness of any Metatarsal
- Types
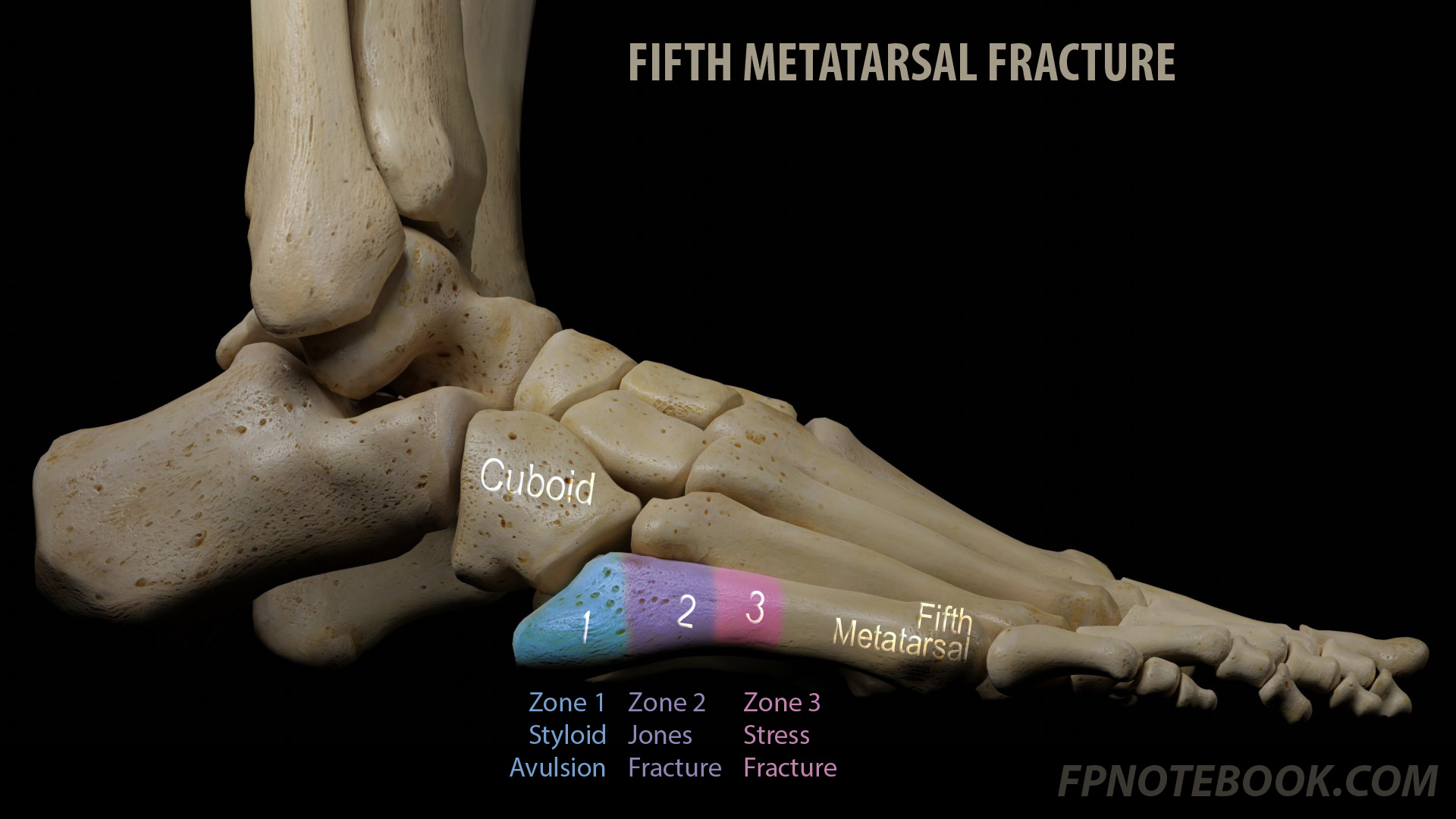
- Based on landmarks along joint between 4th and 5th Metatarsals proximally
- Zone 1: Tuberosity Avulsion Fractures (Styloid Fractures, Pseudo-Jones Fracture, Dancer's Fracture)
- Most common diagnosed lower extremity Fracture (and 90% of Proximal Fifth Metatarsal Fractures)
- Proximal to the joint between 4th and 5th Metatarsals
- Mechanism
- Lateral Ankle Sprain (inversion injury while foot plantar flexed)
- Avulsion injury of the peroneus brevis tendon and plantar aponeurosis
- Typically heal without complications
- Zone 2: Metaphyseal-Diaphyseal Junction Fractures (Jones Fracture)
- Fracture line extends toward the joint between 4th and 5th Metatarsals
- Occurs 1.5 to 3 cm from the tip of the tip of the Metatarsal
- Mechanism: Sudden "cutting" motion side-to-side while the heel is off the ground
- Forceful adduction to plantar flexed foot
- High risk area for non-healing Fractures (non-union)
- Lies in the vascular watershed zone (at risk for poor healing, non-union)
- Fracture line extends toward the joint between 4th and 5th Metatarsals
- Zone 3: Diaphyseal Stress Fractures
- Distal to the joint between 4th and 5th Metatarsals
- Mechanism: Recurrent Trauma such as jumping and pivoting in young athletes (Stress Fracture)
- Insidious pain onset with activity
- Highest risk area for non-healing Fractures (non-union)
-
Metatarsal Shaft Fracture
- Rotational force while foot is in plantar flexion (often accompanying an Ankle Sprain)
- Typically oblique Fractures
- Proximal at medial aspect, to distal at lateral aspect
- Lower risk, and management is more similar to uncomplicated Metatarsal Fractures than to proximal fifth Fractures
- Symptoms
- Distribution: Lateral Foot Pain
- Provocative: Walking
- Timing:
- Acute Fractures: Sudden onset
- Stress Fractures: Gradually progressive and increased with activity
- Signs
- Localized swelling and Ecchymosis at the base of the fifth Metatarsal (or shaft Fracture)
- Imaging
- XRay demonstrates Proximal Fifth Metatarsal Fracture
- See Proximal Fifth Metatarsal Fracture Grading Based on XRay
- See Types above for determining Fracture Type
- Obtain initial 3 view XRay (AP, lateral and oblique)
- Zone 1 imaging repeated in 6 weeks (if persistent pain or symptoms)
- Zone 2 imaging repeated at 2-4 week intervals
- Zone 3 imaging repeated at 4 week intervals
- Fifth Metatarsal Shaft Fracture imaging is repeated in 1-2 weeks and again in 4-6 weeks
- Differential diagnosis on XRay of Proximal Fifth Metatarsal Fracture look-alikes
- Accessory bones (smooth, rounded densities surrounded by cortex)
- Styloid apophysis (children and teens)
- Images
- Indications for orthopedic referral
- Displaced tuberosity avulsion Fractures (>3 mm)
- Nonunion Fractures
- Cuboid-Metatarsal joint with >1-2 mm step-off
- Fracture fragment involves more than 60% of the Metatarsal-Cuboid joint surface
- Protocol for uncomplicated, non-displaced tuberosity avulsion Fractures
- Re-evaluate every 2 to 4 weeks, encouraging mobility
- Option 1
- Soft Bulky Dressing and weight bearing
- Option 2 (if pain despite Option 1)
- Hard soled shoe or cast boot and weight bearing (use for 5-6 weeks)
- Option 3 (if pain despite Option 2)
- Short leg walking boot or cast
- Limit Casting to no more than 2 weeks (longer course risks loss of range of motion)
- Protocol for minimally displaced tuberosity avulsion Fractures (<3 mm)
- Short leg walking boot or cast for 2 weeks
- Progressive ambulation and range of motion follow immobilization
- Reevaluation every 2 weeks and anticipate healing by 4-8 weeks
- Repeat XRay at 6-8 weeks to document healing (sooner if persistent pain on ambulation after 4 weeks)
- Course
- Anticipate asymptomatic by 3-6 weeks (pain may persist up to 8 weeks)
- Anticipate healed with union on XRay by 8 weeks
- Management
- Metaphyseal-Diaphyseal Junction Fractures (Jones Fracture, Zone 2)
- Indications for orthopedic referral
- Consider Consultation in all patients given higher risk of non-union
- Athletes may also benefit from referral by decreasing duration of healing time
- Displacement >2mm
- Inadequate healing after immobilization for 12 weeks
- Non-union on xray
- Initial management
- Options: Non-displaced Jones Fracture (acute diaphyseal Fracture)
- Consider early surgical fixation in athletes
- Non-weight bearing short-leg cast or boot for 6-8 weeks
- Callus formation on follow-up XRay and no point tenderness at 6-8 weeks
- Start weight bearing in CAM Boot and continue for up to 6 weeks (if no pain on ambulation)
- Initiate physical therapy
- Inadequate callus formation on follow-up XRay or point tenderness at 6-8 weeks
- Continue non-weight bearing for additional 4 weeks and re-evaluate
- Callus formation on follow-up XRay and no point tenderness at 6-8 weeks
- Anticipate 6-10 weeks total of immobilization and up to 12 weeks for full healing
- Surgical repair may ultimately be needed in those managed with immobilization
- Management
- Diaphyseal Stress Fractures (Zone 3)
- See Proximal Fifth Metatarsal Fracture Grading Based on XRay
- Indications for orthopedic referral
- See Jones Fracture (Zone 2) referral indications as above
- Most Zone 3 Fractures are referred to orthopedics
- Diaphyseal Stress Fracture Type I (early, See Torg Classification)
- Same management for Jones Fracture above
- Diaphyseal Stress Fracture Type II (delayed, See Torg Classification)
- Early surgical fixation or
- Non-weight bearing cast for up to 20 weeks
- Diaphyseal Stress Fracture Type III (nonunion, See Torg Classification)
- Surgical fixation or
- Non-weight bearing cast for up to 16 weeks and pulsed electromagnetic fields
- References
- Management
- Fifth Metatarsal Shaft Fracture (Non-proximal)
- Initial management
- Immobilize foot in walking boot or hard soled shoe for 4 weeks
- Ambulation as tolerated
-
XRay Imaging Protocol (3 view XRay)
- Imaging is repeated in 1-2 weeks and again in 4-6 weeks
- Referral Indications
- Rotational deformity
- Persistent displacement >3 to 5 mm despite reduction
- Fracture non-union after 6 months
- Compartment Syndrome, Open Fracture or vascular compromise (emergent Consultation)
- References
- Feden and Kiel (2017) Crit Dec Emerg Med 31(11): 3-10
- Bica (2016) Am Fam Physician 93(3): 183-91 [PubMed]
- Hatch (2007) Am Fam Physician 76: 817-26 [PubMed]
- Quill (1995) Orthop Clin North Am 26:353-61 [PubMed]
- Silver (2024) Am Fam Physician 109(2): 119-29 [PubMed]