Peroneal Tendinopathy, Peroneal Tendonitis, Peroneal Tendinitis, Peroneus Longus Tenosynovitis, Peroneus Brevis Tenosynovitis, Peroneus Longus Tendinitis, Peroneus Brevis Tendinitis, Peroneal Tendon Injury
- Physiology
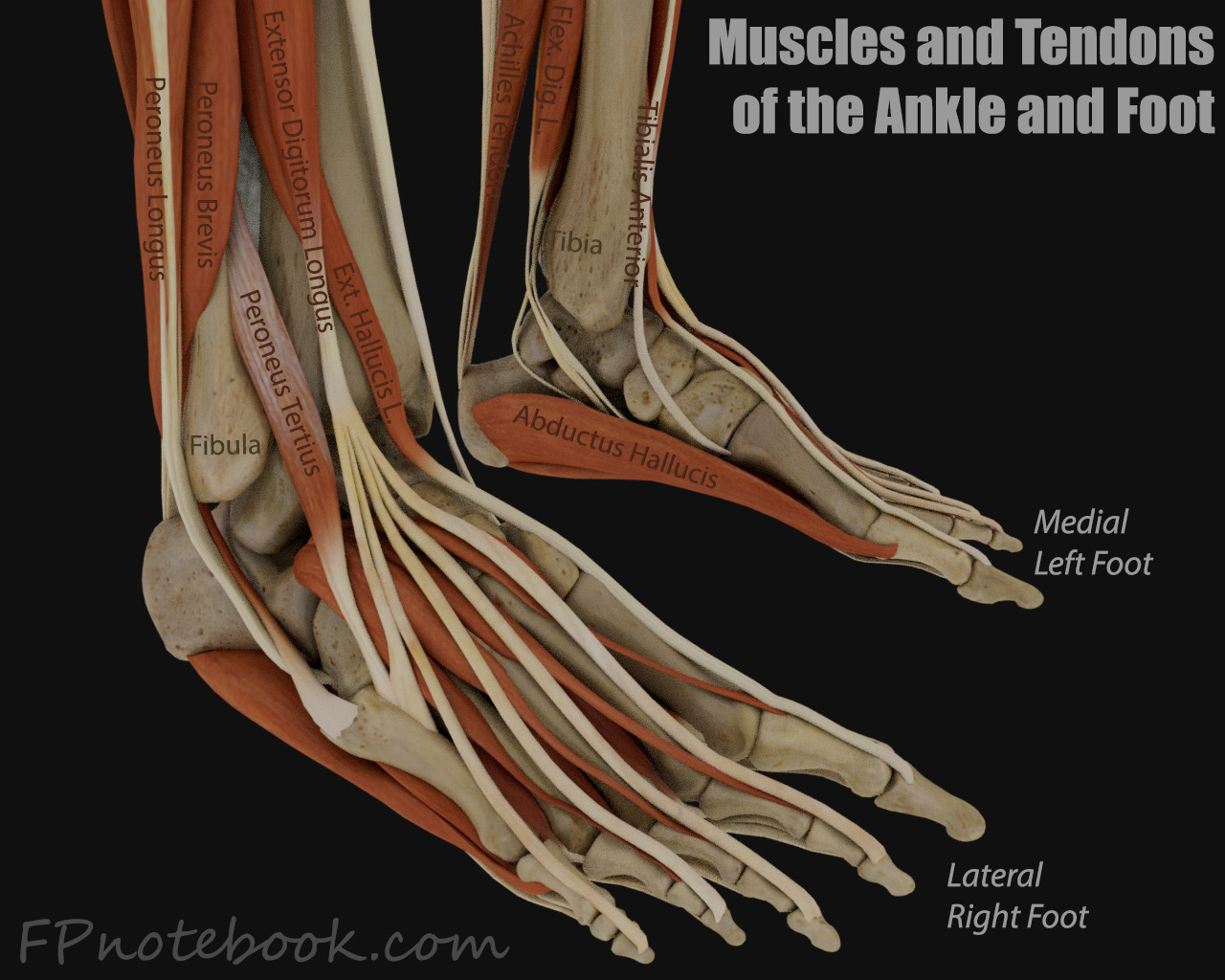
- Peroneus Longus and Brevis act function in ankle eversion and plantar flexion
- Images
- Pathophysiology
- Peroneal Tendon Injury includes peroneal tenosynovitis, subluxation and tendon tears
- Mechanism
- Prolonged or repetitive activity
- Running Injury (overuse)
-
Lateral Ankle Sprain (ankle inversion injury, esp. in first degree sprains)
- Injury may be to Peroneus Longus, or more commonly to Peroneus Brevis
- Risk Factors
- Forefoot striking pattern (esp. Running Injury)
- Medication exposures
- Chronic medical conditions
- Symptoms
- Chronic lateral ankle pain (retrofibular), popping and swelling
- Ankle instability
- Signs
- Observation with patient standing
- Peroneal tendon may be seen contracting, overcoming inversion while maintaining stance
- Hindfoot varus (heel varus) with inverted foot and ankle
- High foot arch
- Cavus foot
- Heel oriented inward
- Palpation
- Pain and swelling posterior to the lateral malleolus at the lateral hindfoot (and over Cuboid tunnel)
- Provocative maneuvers
- Weakness and pain with active motor activity
- Passive stretch foot and ankle in inversion and dorsiflexion
- Positive if painful
- Resisted foot eversion and plantar flexion
- Positive if weak or painful
- Palpate during resistance for tenderness along fibular groove (posterolateral ankle)
- Pain indicates a positive peroneal compression test
- Circumduct ankle
- Observe for peroneal tendon subluxation over the lateral malleolus
- Compress superior peroneal Retinaculum
- Pain and crepitus may be present with peroneus brevis tears
- Differential Diagnosis
- Ankle Sprain
- Fibular Fracture
- Peroneal Subluxation
- Os perineum syndrome (plantar lateral Foot Pain)
- Rheumatoid Arthritis (consider if lack of Trauma)
- Imaging
-
Ultrasound for peroneal instability
- Test Sensitivity: 100%
- Test Specificity: 85%
- MRI
- Consider in suspected peroneus brevis tears (Test Sensitivity: 83%)
- Management
- RICE-M initially
- NSAIDs
- Modify activities
- Rehabilitation Exercises (consider physical therapy referral)
- Ankle Range of Motion
- Peroneal strengthening (Eversion strengthening and progressive loading)
- Proprioception Exercises
- Shoe Orthotic
- Lateral heel wedge to offload peroneal tendons
- First Metatarsal head recessed depression to increase foot valgus
- Heel cushion may offer comfort
- Peroneal Corticosteroid Injection
- Consider in refractory cases
- Appears effective and with low risk of tendon rupture
- Perform under Ultrasound guidance (consider Sports Medicine Referral)
- Fram (2019) Foot Ankle Int 40(8): 888-94 [PubMed]
- Muir (2011) Am J Phys Med Rehabil 90(7): 564-71 [PubMed]
- Immobilization (CAM Boot or Short Leg Walking Cast)
- Consider in refractory cases
- Orthopedic Referral Indications (possible surgical repair)
- Refractory to therapy above
- Inability to bear weight >1 to 2 weeks after injury
- Persistent or recurrent peroneal tendon instability
- Peroneal tendon rupture suspected or confirmed (refer early)
- References
- Sammarco (1994) Orthop Clin North Am 25(1): 135-45
- Deu (2022) Am Fam Physician 105(5): 479-86 [PubMed]
- Morancie (2025) Am Fam Physician 112(6): 648-56 [PubMed]
- Simpson (2009) Am Fam Physician 80(10): 1107-13 [PubMed]