Calcaneal Apophysitis, Sever's Disease, Sever Disease, Calcaneoapophysitis, Apophysitis of the Achilles Tendon
- Epidemiology
- Pathophysiology
- Traction Apophysitis at posterior Calcaneus in competitive child and teen athletes with immature skeletons
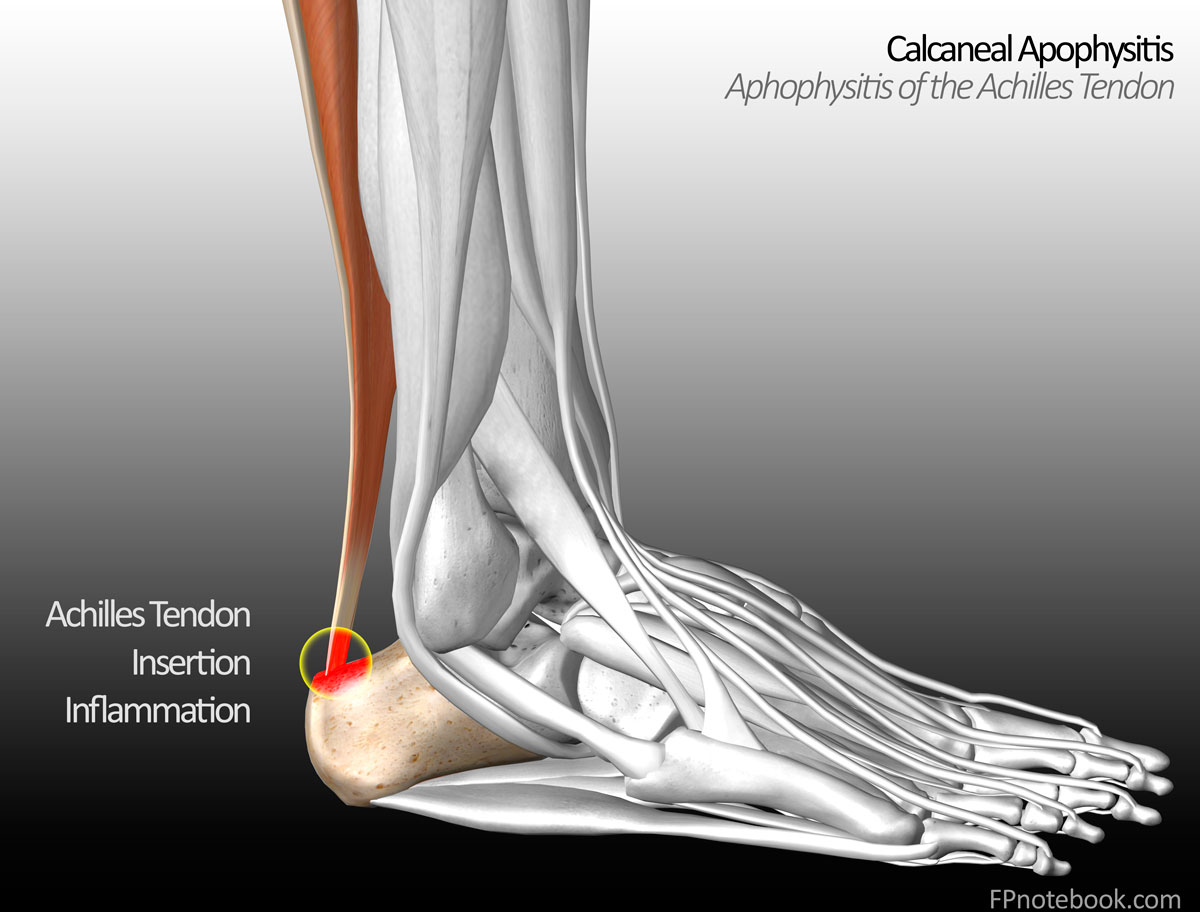
- Low grade inflammation and Apophysitis at achilles tendon insertion
- Associated with irregular ossification
- Sclerosis of calcaneal apophysis
- Images
- Mechanism
- Traction injury of the achilles tendon insertion at the Calcaneus
- Risk Factors
- Tight heel cord
- Running or jumping sports
- Early sports specialization
- Symptoms
- Heel Pain with insidious onset (bilateral in 60% of cases)
- Ambulation is not painful (but weight bearing may exacerbate the pain)
- Posterior Calcaneus pain
- Pain worse during or after high impact activity, and improves with rest
- Wearing shoes is painful (esp. soccer cleats)
- Pain is worse at the begining of a season or during a growth spurt
- Signs
- Point tenderness over the achilles tendon insertion
-
Calcaneus inflammation
- Achilles tendon pain and tenderness at the Calcaneus insertion
- Swelling may be present
- Tight heel cord
- Passive dorsiflexion of heel cord reproduces pain
- Provocative Testing (>95% Test Sensitivity and Test Specificity)
- Calcaneal Squeeze Test (medial and lateral compression of Calcaneus)
- One legged heel standing
- Differential Diagnosis
- Imaging
- Foot XRay
- Indications
- Severe symptoms or refractory cases (e.g. >8 weeks)
- Typically normal
- May demonstrate sclerosis of calcaneal apophysis
- However sclerosis also seen in normal, asymptomatic feet
- Evaluate for alternative diagnoses (e.g. Calcaneal Stress Fracture)
- Management
-
General Measures
- NSAIDs or Acetaminophen
- Local heat
- Ice Therapy
- Relative Rest
- Limit activity to pain free sports during recovery
- Physical Therapy
- Calf and Heel Cord StretchingExercises
- Focus on gastrocnemius Muscle and soleus muscle Stretching
-
Orthotics
- Available as off-the-shelf products, but custom Orthotics are most effective
- Padded heel cup
- Heel lift (1.25 cm)
- Diminishes heel cord stress
-
Short Leg Walking Cast (resistant cases)
- Foot in slight equinus (plantar flexion)
- Course
- Anticipate return to activity within 6 weeks
- Anticipate full recovery within 2 months
- Prognosis
- Self limited condition with good overall prognosis
- Typically resolves with Epiphyseal Plate closure at age 15 to 16 years old
- References
- Achar (2019) Am Fam Physician 99(10): 610-8 [PubMed]
- Atanda (2011) Am Fam Physician 83(3): 285-91 [PubMed]
- Lintner (2023) Am Fam Physician 108(6): 544-553 [PubMed]
- Madden (1996) Am Fam Physician 54(6):1995-2000 [PubMed]
- Morancie (2025) Am Fam Physician 112(6): 648-56 [PubMed]
- Ogden (2004) J Pediatr Orthop 24(5): 488-92 [PubMed]
- Tu (2018) Am Fam Physician 97(2):86-93 [PubMed]