Adjustable Gastric Banding, Laparoscopic Adjustable Gastric Banding, Adjustable Gastric Banding Surgery, Gastric banding
- See Also
- Indications
- Morbid Obesity
- Epidemiology
- Most common form of Bariatric Surgery in U.S.
- Background
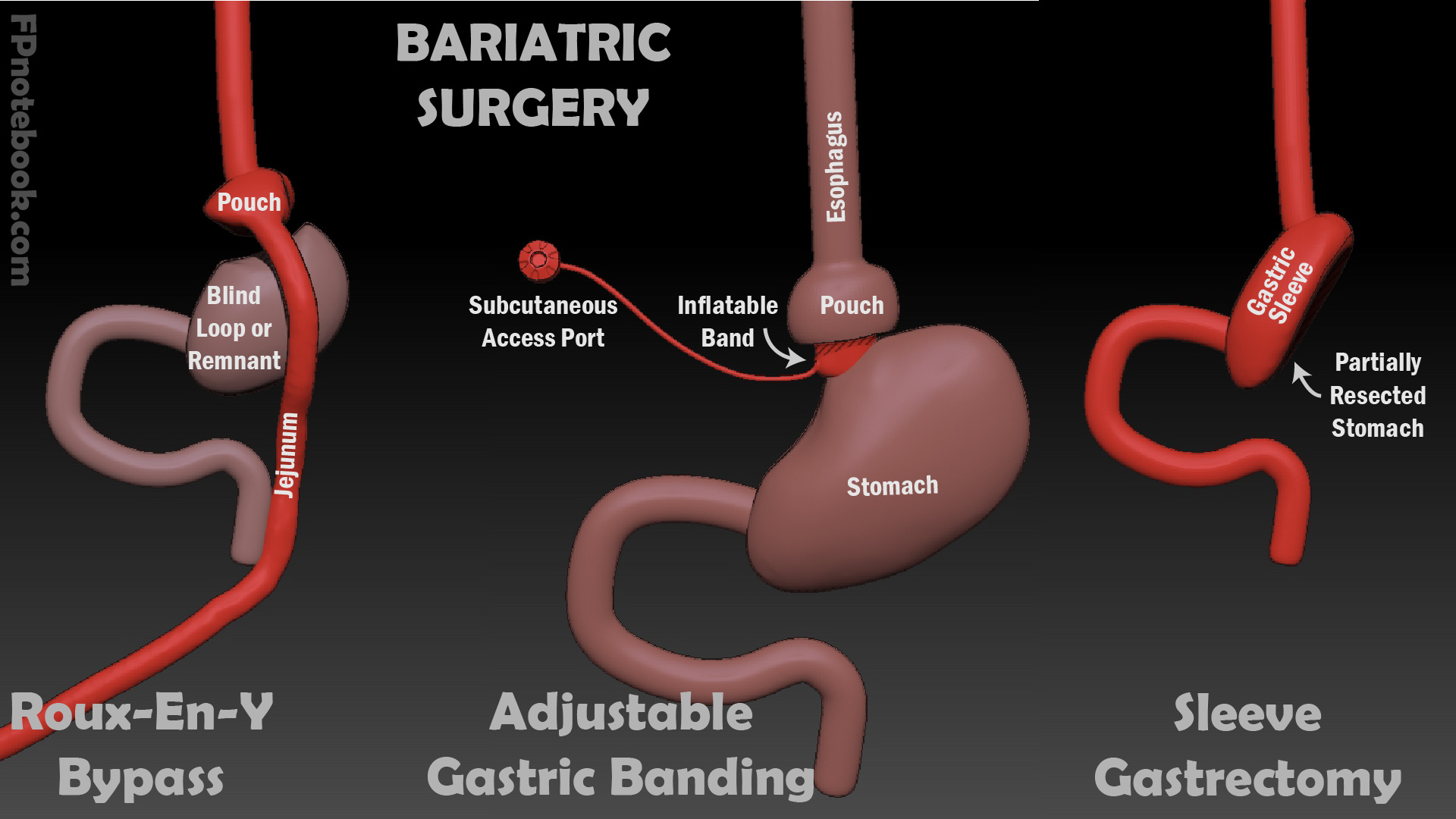
- Images
- Introduced in 2006
- Band applied around the distal Esophagus or proximal Stomache
- Reversible and tension can be adjusted via subcutaneous port
- Replaces Vertical Banded Gastroplasty
- Efficacy
- Weight loss 21% at 1 year and 13% at 10 years
- Prognosis
- Outcomes
- Reoperation is required in 50% of cases
- Major late complication rate: 25%
- Dissatisfaction with surgery (would not choose it again): 73%
- Complications
- Failed Weight Loss (<20% of excess weight lost)
- Diet evaluation
- Meal volume
- Between meal snacks
- Excess liquid calories
- Band Evaluation
- Evaluate for band leakage
- Complications
- Early Postoperative (<1 month postoperative)
- See Bariatric Surgery
- Life threatening
- Common
- Infection
- Stomal stenosis
- Hernia
- Complications
- Gastric Band Slippage
- Risk Factors
- Overeating
- Earlier procedure prior to pars flacida technique
- Prior to this technique posterior band slippage was more common
- Presenting symptoms
- Step 1: Diagnosis
- Imaging Studies
- Abdominal XRay
- Upper gastrointestinal contrast (Gastrograffin Upper GI Series)
- Imaging suggests pouch dilation
- Reinforce dietary management
- Imaging suggests band slippage
- Go to Step 2
- Imaging Studies
- Step 2: Gastric Band Slippage confirmed
- Deflate gastric band urgently
- Symptoms improve
- Routine follow-up
- Symptoms persist but are stable
- Reinforce dietary management
- Consider gastric band removal
- Symptoms persist and worsen
- Go to Step 3
- Step 3: Surgical evaluation (laparoscopy, laparotomy)
- Band slippage with full thickness erosion, necrosis or abscess
- Gastric band removal AND
- Excision of affected tissue
- Band slippage without erosion or necrosis
- Gastric band removal OR
- Unbuckle band
- Band slippage with full thickness erosion, necrosis or abscess
- References
- Complications
- Port or tubing malfunction
- Causes
- Leakage of saline (saline keeps band inflated)
- Port rotation or migration
- Presentations
- Inability to access port
- Inadequate weight loss or regained weight
- Evaluation
- Device evaluation under fluoroscopy
- Management
- Endoscopic port replacement or
- Intra-abdominal surgical correction
- Complications
- Pouch dilation
- Causes
- Band overinflation
- Overeating
- Presentations
- Loss of satiety
- Gastroesophageal Reflux or regurgitation
- Management: Initial
- Deflate band
- Reinforce dietary management
- Management: Re-evaluate at 4-6 weeks
- Anticipate pouch size return to normal in 4-6 weeks
- Consider gastric band replacement or removal
- Complications
- Port site prominence
- Weight loss results in decreased subcutaneous fat
- Port rubs on overlying clothing resulting in irritation, pain and Skin Erosions
- Consider port replacement (smaller, low profile)
- Complications
- Stomal obstruction
- Gastric pouch outlet obstruction
- Causes
- Swallowing large food boluses
- Presentation
- Dysphagia
- Reflux
- Postprandial Vomiting
- Abdominal Pain
- Management
- Attempt to correct with band deflation or endoscopic release of obstruction
- Gastric band removal if other corrective measures not effective
- Complications
- GERD
- Causes
- Hiatal Hernia (consider repair prior to Gastric banding)
- Pouch dilation
- Noncompliant with dietary management
- Management
- Reinforce dietary management
- Proton Pump Inhibitor (or other acid suppression)
- Surgical management (e.g. gastric band removal) if refractory to other measures
- Complications
- Port Infection
- Early
- Local tenderness, warmth, redness
- Late
- Abscess or fistula formation (with Abdominal Pain or failed weight loss)
- Diagnosed by exam, Ultrasound or endoscopy
- Complications
- Band Erosion
- Presentation
- Weight gain
- Abdominal Pain
- Dysphagia
- Hematemesis
- Sepsis
- Abscess at port site (migrating from Stomach)
- Diagnosis
- Upper GI Study
- Abdominal CT
- Management
- Band removal (may be replaced at 3 months)
- Gastric wall repair