Electrocardiogram in Myocardial Infarction, EKG in Acute MI, EKG in Myocardial Ischemia, EKG in Cardiac Ischemia, EKG Markers of Underlying Coronary Artery Disease, EKG in Acute Coronary Syndrome, Septal Myocardial Infarction EKG Changes, Anterior Myocardial Infarction EKG Changes, Anteroseptal Myocardial Infarction EKG Changes, Anterior Myocardial Ischemia EKG Changes, Inferior Myocardial Infarction EKG Changes, Inferior Myocardial Ischemia EKG Changes, Lateral Myocardial Infarction EKG Changes, Lateral Myocardial Ischemia EKG Changes, Posterior Myocardial Infarction EKG Changes
- See Also
- Advantages
- Ischemic EKG changes best acute MI evidence
- Applies if symptom onset within last 3 hours
- Normal/Nondiagnostic initial EKG predicts low risk
- Disadvantages
- Poor sensitivity for Myocardial Infarction (40-50%)
- 3-10% of MI patients have initial normal EKG
- 25% of patients with missed MI had misread EKG
- Precautions
- The computer over-reads abnormal EKGs
- Compare with prior EKGs (Increases Test Specificity)!
- Obtain serial EKGs if initial EKG is non-diagnostic
- May repeat EKG every 15 min for 1-2 hours
- Consider Myocardial Ischemia if ST depression >0.5 mm
- Images
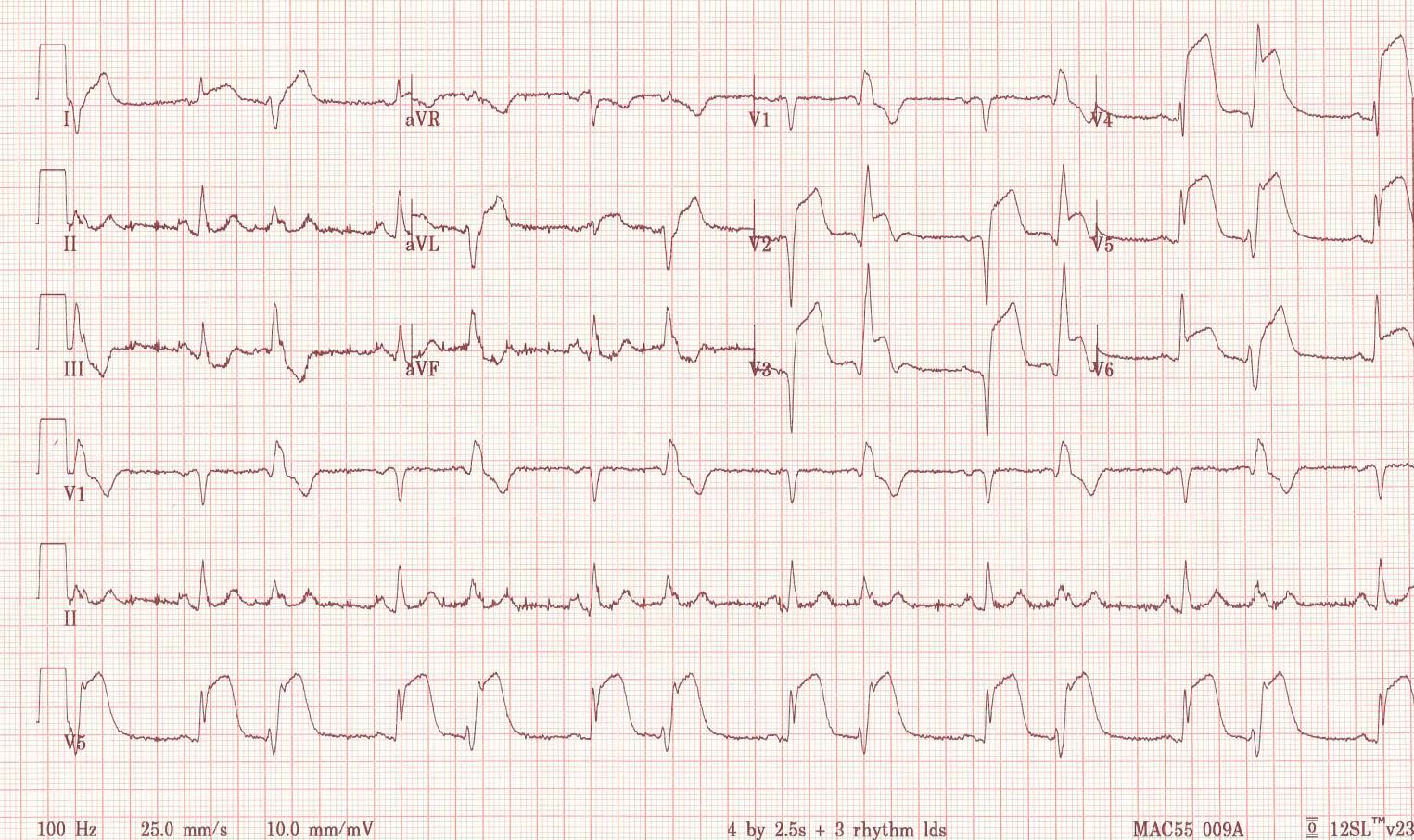
- Acute ST Elevation Myocardial Infarction with delayed presentation (ST Elevation and Q Waves present)
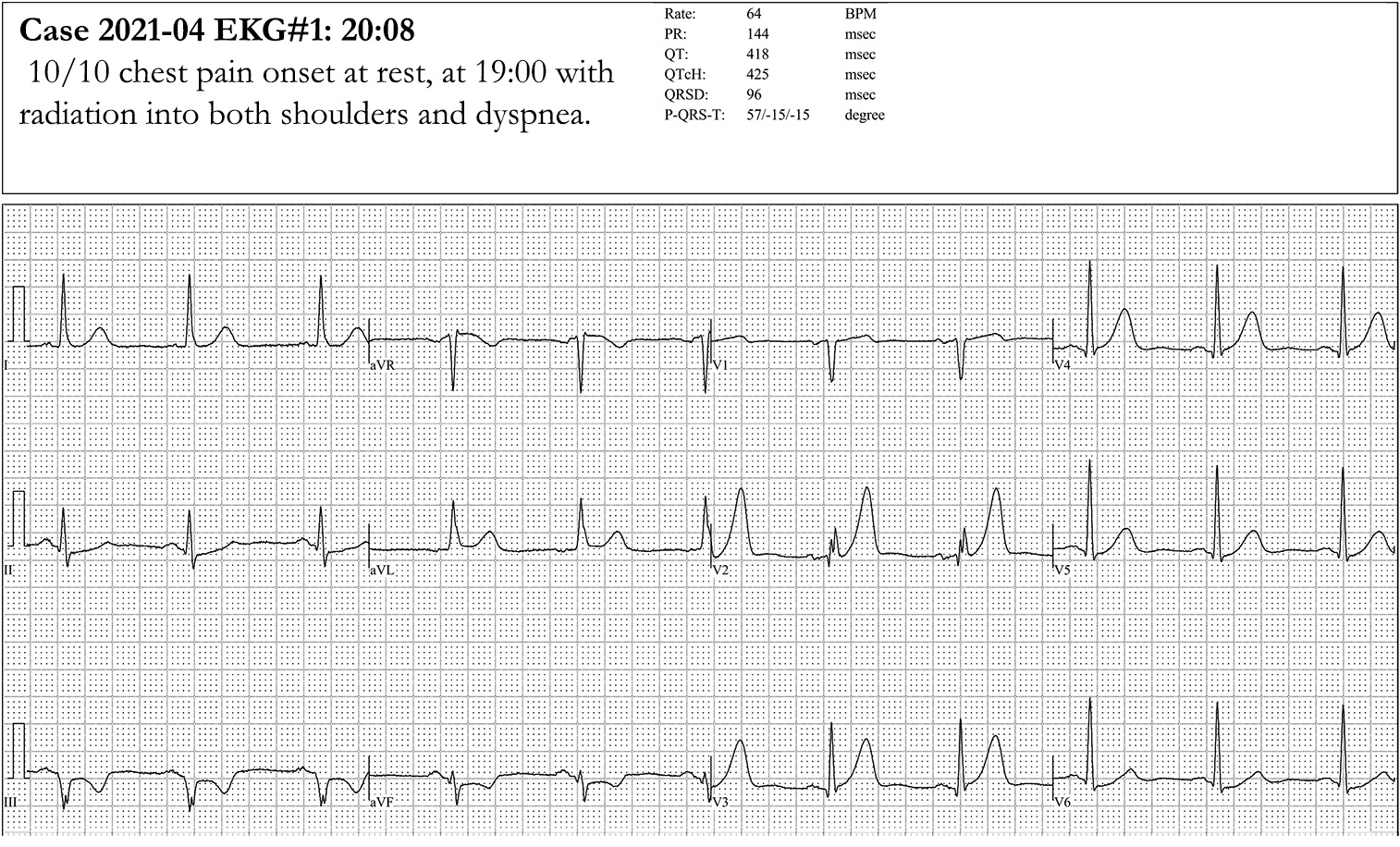
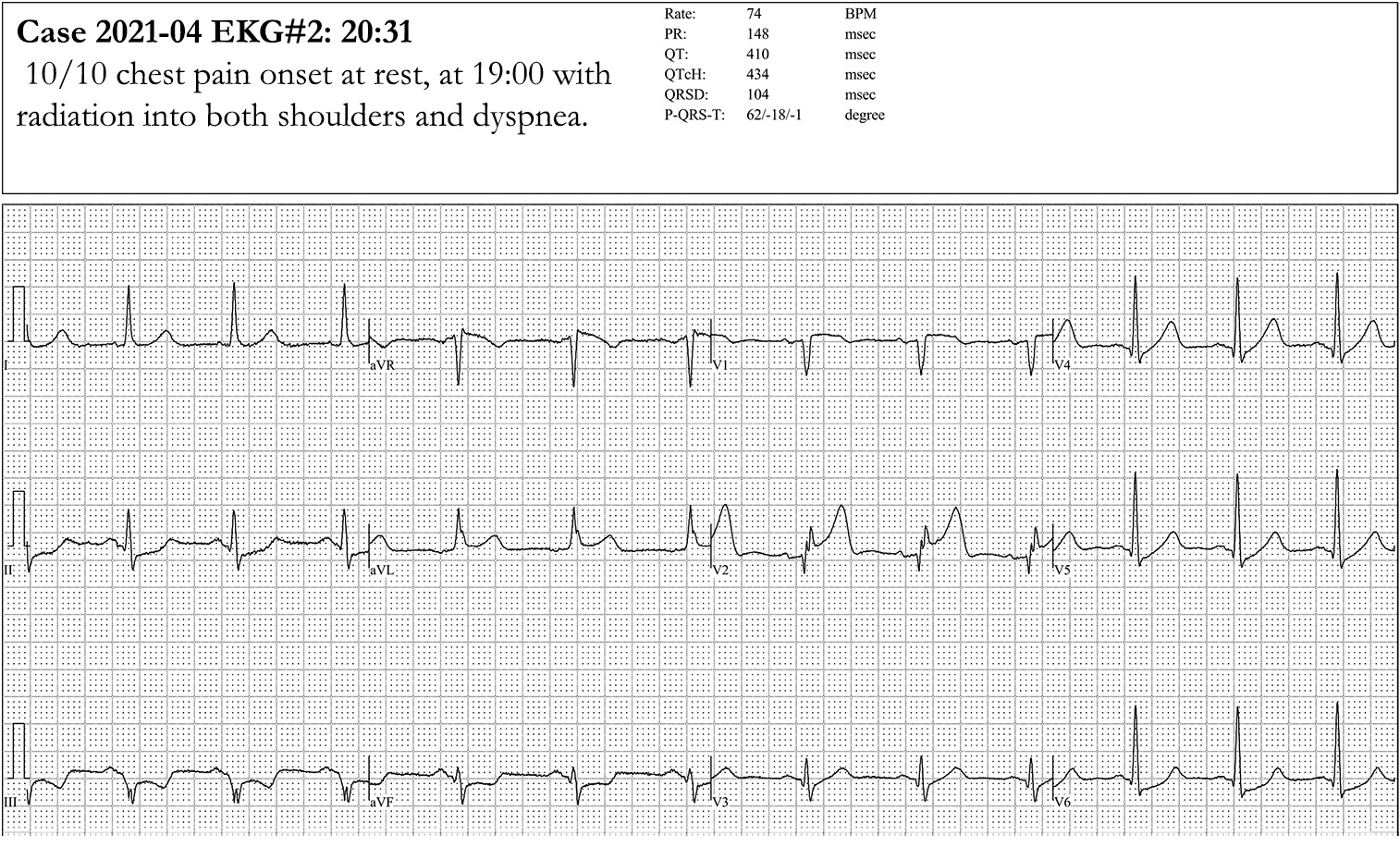
- Acute ST Elevation Myocardial Infarction evolving from Hyperacute T Waves
- Findings
- EKG Markers of underlying CAD
- Left Ventricular Hypertrophy
- ST Segment changes
- T Wave changes
- Diagnostic Q Waves in 2 contiguous leads
- Left Bundle Branch Block or other conduction changes
- Findings
- General EKG Changes suggestive of Myocardial Ischemia
- Electrocardiogram may be completely normal
-
ST Elevation or ST depression
- Over 1 mm ST changes that are transient with symptoms
- Summed ST deviation (sum of affected leads) >2.5 mm
- ST Elevation criteria in leads V2-V3 varies by age and gender
- Men age <40 years old
- V2-V3 ST Elevation >2.5 mm
- Accounts for Early Repolarization in young men
- Men age >40 years old
- V2-V3 ST Elevation >2 mm
- Women
- V2-V3 ST Elevation >1.5 mm
- Men age <40 years old
- Deep symmetric T-wave inversion
- Occurs in multiple precordial leads
- Left main Coronary Artery stenosis marker
- ST Depression >1 mm in 8 or more leads (esp I, II, V4-6) AND ST Elevation in aVR, aVL or V1
- Suggests multi-vessel ischemia or left main obstruction
- aVR ST Segment Elevation > V1 ST Segment Elevation
- Biphasic or Deep T Wave Inversion in V2, V3 (Wellen's Syndrome)
- High risk for left anterior descending artery ischemia and Anterior Wall Myocardial Infarction
- ST Depression >1 mm in 8 or more leads (esp I, II, V4-6) AND ST Elevation in aVR, aVL or V1
- Left Anterior Descending Artery Occlusion
- Hyperacute T Waves with J Point Depression (De Winter T Waves, seen in 2% of LAD lesions)
- J Point depression with upsloping ST Segment AND
- Tall, prominent, hyperacute precordial T Waves
- Hyperacute T Waves also seen in Hyperkalemia, STEMI without J Point depression
- Hyperacute T Waves with J Point Depression (De Winter T Waves, seen in 2% of LAD lesions)
- Findings
- General EKG Changes suggestive of Acute Myocardial Infarction
- New left ventricular strain pattern
-
New Left Bundle Branch Block
- Sgarbossa Criteria and Modified Sgarbossa Criteria may identify STEMI despite Left Bundle Branch Block (or right ventricular Pacemaker)
-
Q Waves
- At least 0.04 sec wide and 1/3 height of R Wave
- Unless isolated in Lead III
-
T Wave Inversion
- Significant unless isolated to Lead III or Lead V1
- T Wave must be at least 1 mm deep
- T Wave Inversion within 4 hours of reperfusion is a reassuring prognostic sign
- ST-T elevation (>1mm in limb or precordial leads)
- Must have >=2 concordant leads with changes
- ST depression in Lead V1, Lead V2 (Posterior MI)
-
Hyperacute T Waves (over 50% of preceding R)
- Must have 2 or more leads with changes
- Findings
- Septal MI Anatomic Distribution
-
Electrocardiogram Changes
- Lead V1 to lead V2
- Distribution
- Left Coronary Artery: LAD-Septal Branch
- Complications
- Infranodal and Bundle Branch Block
- Findings
- Anterior MI Anatomic Distribution
- EKG Changes
- ST Elevation in lead V2 to lead V4
- ST depression in leads II, III, avF (variably present)
- Distribution
- Left Coronary Artery: LAD-Diagonal branch
- Complications
- Worse prognosis
- High risk of sudden death
- High risk of Congestive Heart Failure in first year
- Complete Heart Block
- Findings
- Inferior MI Anatomic Distribution
- EKG Changes
- ST Elevation in leads II, III, aVF
- Q Waves in leads III, aVF
- ST depression and T Wave Inversion in lead aVL (reciprocal change)
- Distribution
- Right Coronary Artery: Posterior descending branch
- Complications
- Right Ventricular Infarction
- Inferior heart wall lies along the diaphragm
- Distended neck veins with clear lungs
- Systolic Blood Pressure drops with
- Right Ventricular Infarction
- Findings
- Lateral MI Anatomic Distribution
- EKG Changes
- ST Segment Elevation in leads V5, V6, I, aVL
- I and aVL are considered contiguous leads (high lateral wall)
- ST Elevation in both I and aVL is considered STEMI criteria for immediate reperfusion
- ST segment Depression in leads V1, V2, V3, III, aVF (reciprocal change)
- ST Segment Elevation in leads V5, V6, I, aVL
- Distribution
- Left Coronary Artery: Circumflex branch
- Complications
- Left Ventricular Dysfunction
- AV nodal block
- Findings
- Right Ventricular Infarction Anatomic Distribution
- Standard EKG Changes (similar to anterior MI EKG when rotated 180 degrees)
- ST Elevation in leads I and aVF, and lead III more than II
- ST depression in leads I, aVL (reciprocal to posterior changes)
- Right sided EKG
- Right Lead Positioning
- Alternative: V4R
- Simply move V4 lead to the right chest (5th intercostal space, mid-clavicular line)
- Findings
- ST Elevation >1mm in V4R
- Q Waves are normal in right-sided leads and are not indicative of Myocardial Infarction history
- Distribution
- Right Coronary Artery: Proximal branches
- Complications
- Severe and refractory Hypotension in response to nitrates
- Treated with fluid bolus and nitrates are contraindicated
- Severe and refractory Hypotension in response to nitrates
- Findings
- Posterior Infarction Anatomic Distribution
- Standard EKG Changes
- ST depression in leads V1 to V4
- Differentiate from reciprocal changes in inferior-lateral MI
- Contrast with right sided infarct with ST Elevation in V1 to V4
- Tall R Wave (>0.04 seconds) in leads V1 and V2
- Interpret V2 by rotating the axis 180 degrees (or apply posterior leads)
- Tall R Wave rotates to a Q Waves
- ST depression rotates to ST Elevation
- T Wave rotates to T Wave Inversion
- ST depression in leads V1 to V4
- Posterior EKG Changes
- Leads V8 and V9 (placed on left back, below left Scapula) demonstrate ST Elevation
- ST Elevation in V8 and V9 posterior leads may be significant at 0.5 mm
- Distribution
- Distal Right Coronary Artery: Posterior descending
- Left Coronary Artery: Circumflex
- Complications