Atrioventricular Reciprocating Tachycardia, Re-entrant Atrioventricular Tachycardia, AVRT, Orthodromic Atrioventricular Re-entrant Tachycardia, Orthodromic AVRT, Antidromic AVRT, Antidromic atrioventricular re-entrant tachycardia
- See Also
- Paroxysmal Supraventricular Tachycardia
- Supraventricular Tachycardia
- Atrioventricular Nodal Reentry (AVNRT)
- Atrial Tachycardia
- Unstable Tachycardia
- Sinus Tachycardia
- Atrial Fibrillation
- Unstable Tachycardia
- Narrow Complex Tachycardia
- Wide Complex Tachycardia
- Cardiopulmonary Resuscitation
- Supraventricular Tachycardia Management in the Child
- Supraventricular Tachycardia Management in the Adult
- Definitions
- Atrioventricular Reciprocating Tachycardia (AVRT)
- Form of Paroxysmal Supraventricular Tachycardia (30% of cases) with an accessory pathway (outside the AV Node)
- Epidemiology
- Overall, second most common cause of PSVT (30% of cases)
- Most common in children (represents 60% of SVT cases in first decade of life)
- Decreasing Prevalence with age (represents 9% of SVT cases over age 70 years)
- Pathophysiology
- Findings
- EKG
- Heart Rate 160 to 240 (up to 256)
- Images
- Types
- General
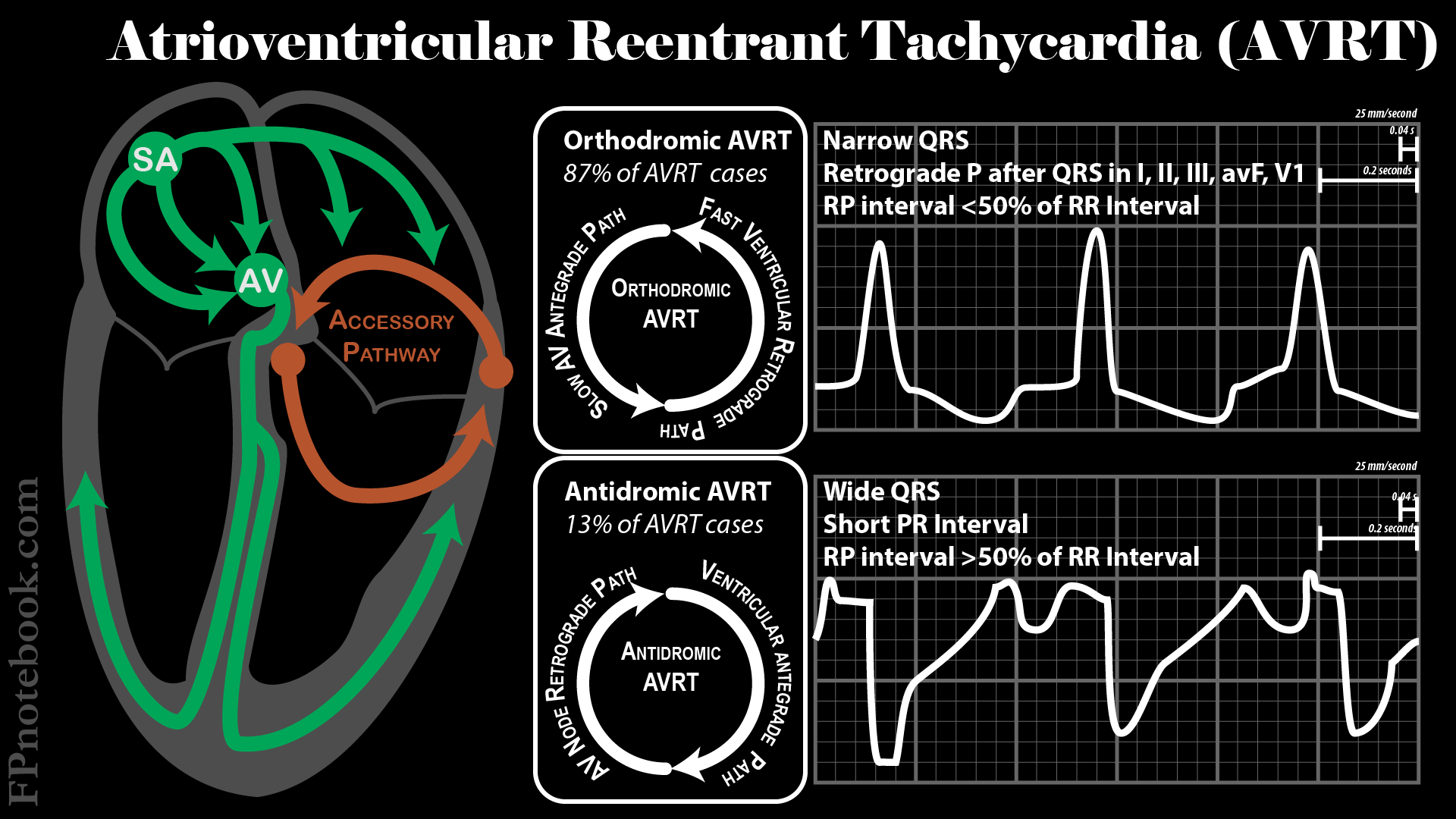
- Orthodromic, narrow complex (87% of cases)
- Signal passes anterograde down the AV Node, through the ventricles and retrograde up the accesory path
- Represents up to 87% of AVRT cases
- Narrow Complex Tachycardia at 150 to 250 bpm
- RP interval is <50% of the tachycardic RR interval
- Retrograde P Waves appear after the QRS in I, II, III, aVF, V1 (may be obscured by T Wave)
- Antidromic, wide complex
- Signal passes retrograde up the AV Node and anterograde down the accessory path
- Wide Complex Tachycardia at 150 to 200 bpm
- RP interval is >50% of the tachycardic RR interval (<100 msec)
- Short PR Interval
- Types
- Variants
-
Wolff-Parkinson-White Syndrome (WPW Syndrome)
- Orthodromic variant
- Anterograde conduction down the accessory path reaches the ventricle before the AV Nodal signal
- Results in preexcitation of the ventricle, forming a slurred upstroke of the QRS (delta wave)
- Permanent (or persistent) Junctional Reciprocating Tachycardia
- Slow retrograde conduction via the accessory pathway
- Results in sustained Supraventricular Tachycardia
- Risk of Tachycardia induced Cardiomyopathy and Congestive Heart Failure
- Management
- Catheter Ablation (preferred)
- First-Line Management for recurrent AVRT
- Medical Management (alternative)
- See Paroxysmal Supraventricular Tachycardia
- See Supraventricular Tachycardia
- Orthodromic AVRT
- Contraindications to AV Nodal and Rate Control Agents
- Preexcitation such as WPW Syndrome (refer for ablation)
- Heart Failure with Reduced Ejection Fraction (HFrEF)
- Medications
- Beta Blocker (e.g. Metoprolol)
- Nondihydropyridine Calcium Channel Blocker (e.g. Diltiazem)
- Contraindications to AV Nodal and Rate Control Agents
- Antidromic AVRT
- Contraindications to Antiarrhythmic Agents
- Ischemic or structural heart disease
- Medications
- Contraindications to Antiarrhythmic Agents
- Course
- May degenerate into Atrial Fibrillation
- References
- Joshi and Dermark (2016) Crit Dec Emerg Med 30(8):3-12
- Colucci (2010) Am Fam Physician 82(8): 942-52 [PubMed]
- Delacretaz (2006) N Engl J Med 354(10): 1039-51 [PubMed]
- Helton (2015) Am Fam Physician 92(9): 793-800 [PubMed]
- Kumar (2006) Cardiol Clin 24(3): 427-37 [PubMed]
- Nasir (2023) Am Fam Physician 107(6): 631-41 [PubMed]