Metatarsus Adductus, Metatarsus Varus, Forefoot Adduction
- See Also
- Definitions
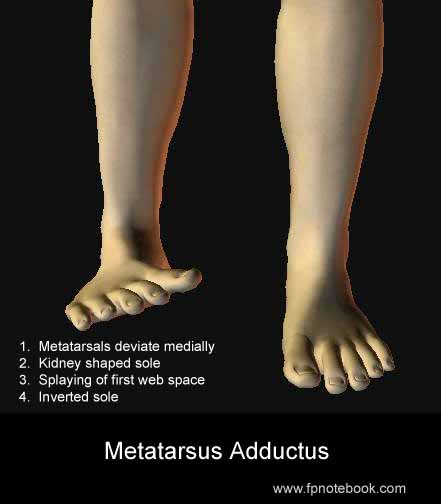
- Metatarsus Adductus
- Forefoot Adduction most commonly at the tarsometatarsal joint, in relation to the hindfoot
- Epidemiology
- Most common congenital foot deformity (present at birth)
- Incidence: 1-2 per 1000 live births
- No gender predominance (affects boys and girls equally)
- Left-side more commonly affected than right
- Pathophysiology
- Among the causes of In-Toeing
- Forefoot Adduction most commonly at the tarsometatarsal joint (Lisfranc Joint), in relation to the hindfoot
- Caused by in-utero confinement
- Higher rtisk in first pregnancies, twin pregnancies and late-term pregnancies (>40 weeks)
- Types
- Metatarsus Adductus (Category A and B)
- Corrects spontaneously by age 3 months in 90% cases
- Associated with medial foot soft tissue contractures
- Flexible deformity
- Forefoot can be rotated at least to neutral position
- Degree of flexibility determines management (see below)
- Metatarsus Varus (Category C)
- Does not spontaneously correct
- Fixed deformity
- Concurrent tarsometatarsal joint medial subluxation
- Signs
- Images
-
General
- Bilateral or Unilateral
- Forefoot rotated inwardly
- Line bisecting heel pass lateral to third toe
- Banana shaped or C-shaped foot
- Lateral border of foot convex
- Medial border of foot concave
- Base of fifth Metatarsal (styloid) prominent
- V-Finger Test
- Infant's heel in examiner's hand second webspace
- Medial foot rests against index finger
- Lateral foot rests against middle finger
- Foot observed from plantar aspect
- Observe for medial deviation of forefoot
- Forefoot deviates away from middle finger
- Infant's heel in examiner's hand second webspace
- Severity
- Assess as flexible versus rigid
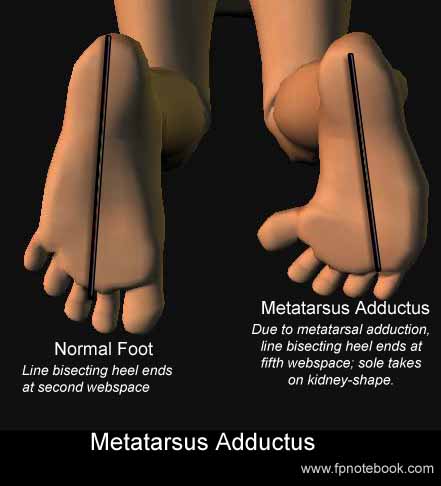
- Heel bisector line drawn from midline heel to forefoot
- Normally bisector line intersects the second toe
- Mild to moderate cases intersect the third or fourth toe
- Severe cases intersect the fourth or fifth toes
-
Newborn Exam
- Heel deviates laterally
- Medial malleoli are further from each other
- Sole deviates medially (Kidney shaped)
- Both feet are inverted (face each other)
- Foot easily dorsiflexed (no tight heel cord in contrast to Clubfoot)
- Document Severity at Newborn Exam
- Based on flexibility of abducting forefoot
- Category A: Mild or flexible
- Category B: Moderate or fixed
- Category C: Severe or rigid
- Heel deviates laterally
- Two month exam: Hold infant in standing position
- Accentuates deformity
- Estimates degree of deformity
- Associated Conditions
- Congenital dislocation of the hip (2-10%)
- Windblown feet
- Both feet point in same direction
- Calcaneovalgus foot on one side
- Metatarsus Varus on other foot
- Differential Diagnosis
- See In-Toeing
- Excessive Femoral Anteversion (most common)
- Medial Tibial Torsion
-
Clubfoot
- Foot also inverted with Forefoot Adduction
- Distinguish by limited ankle extension (equinus)
- Prognosis
- Mild or flexible improves during first 3 months of life
- Suggests Metatarsus Adductus
- Full resolution spontaneously in 85% of cases
- Rigid deformity requires treatment
- Prevents complications in adults
- Adult Bunions and calluses at fifth Metatarsal
- Management
- Category A: Mild/flexible deformity (Most common)
- Flexible
- Forefoot can abduct past the midline of the heel bisector angle
- Resolves spontaneously in most cases (and those that persist are typically asymptomatic)
- Semi-Flexible (partial)
- Forefoot can abduct to the midline of the heel bisector angle
- Refer to pediatric orthopedics if unresolved at age 1-2 years
- Parents may stretch child's foot
- Firmly stabilize heel
- Stretch forefoot laterally (everting foot)
- Hold for count of 5 (baby will wince, not cry)
- Do for 5 repetitions at each diaper change
- Flexible
- Category B: Moderate/fixed deformity
- Evaluation by pediatric orthopedics
- May be associated with metatarsus primus varus
- Results in extreme adduction of the great toe
- May make application of shoes and socks difficult
- Surgical release of abductor hallucis
- Perform at 6 to 18 months
- Category C: Severe/rigid deformity (rare)
- Serial casts (or adjustable shoes in pre-walking infants) in first few weeks of life
- Takes advantage of neonates ligament laxity
- Corrective Surgery if above not effective (2-4 years old)
- Age <7: Soft tissue release tarsometatarsal joint
- Age >7: Metatarsal Osteotomy
- Serial casts (or adjustable shoes in pre-walking infants) in first few weeks of life
- Prognosis
- Spontaneous resolution in 85-90% of cases by age 1 year
- Only 4% of cases remain at age 16 years
- Often persistent Metatarsus Adductus is asymptomatic, even in adults
- Patient Resources
- Hughston Sports Medicine Foundation
- References
- Bates (1991) Physical Exam, Lippincott
- Hoppenfeld (1976) Exam. Spine Extremities, p.159-60,223
- Pediatric Database Homepage by Alan Gandy, MD
- Baird (2025) Am Fam Physician 111(2): 125-39 [PubMed]
- Churgay (1993) Am Fam Physician 47(4):883 [PubMed]
- Gore (2004) Am Fam Physician 69(4):865-72 [PubMed]
- Hoffinger (1996) Pediatr Clin North Am 43:1091-111 [PubMed]
- Rerucha (2017) Am Fam Physician 96(4): 226-33 [PubMed]
- Sass (2003) Am Fam Physician 68(3):461-8 [PubMed]