Clubfoot, Talipes Equinovarus
- Epidemiology
- Often Bilateral
- Hereditary
- Incidence: 1-2 per 1000 live births
- More common in hispanic patients
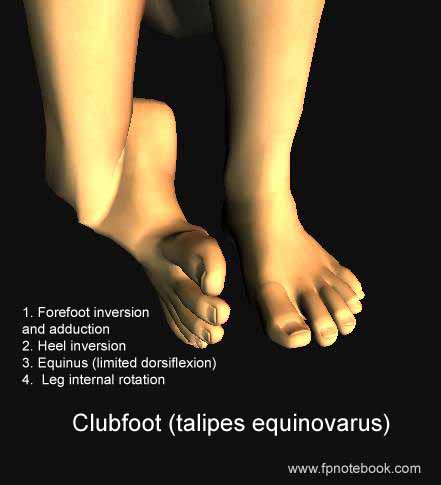
- Signs (4 components)
- Foot is down and in
- Images
- Heel inversion (varus) with internal rotation
- Medial malleoli are further from each other
- Forefoot inverted and adducted (soles face each other)
- Plantar flexion with inability to dorsiflex
- Equinus of Ankle and forefoot
- Very tight heel cord
- Leg internal rotation
- Associated deformity
- Congenital dislocation of Hip
- Spina bifida
- Myotonic Dystrophy
- Arthrogryposis
- Types
- Extrinsic Clubfoot (Mild, Supple form)
- Secondary to intrauterine compression
- Intrinsic Clubfoot (Severe, Rigid form)
- Anatomic deformity (e.g. abnormal talus)
- Differential Diagnosis
- Metatarsus Adductus (foot not in equinus)
- Management
- Refer immediately for serial casts
- Serial Casting
- Start in first week of life
- Serial Casts weekly for 6-8 weeks
- Take advantage of neonatal ligamentous laxity
- Manipulate foot before and between casts
- Stretches contracted soft tissues
- Casting is most effective in extrinsic Clubfoot
- Dennis-Browne Splines
- Goal is a flat, platform-like base for ambulation
- Severe Clubfoot requires surgery
- Posteromedial release of heel cords
- Major surgery in 50-75% cases
- Patient Resources
- Hughston Sports Medicine Foundation
- References
- Hoppenfeld (1976) Exam. Spine Extremities, p.159-60,223
- Churgay (1993) Am Fam Physician 47(4):883 [PubMed]
- Gore (2004) Am Fam Physician 69(4):865-72 [PubMed]
- Hoffinger (1996) Pediatr Clin North Am 43:1091-111 [PubMed]