Lisfranc Fracture Dislocation, Closed Fracture Dislocation of Tarsometatarsal Joint, Lisfranc Fracture, Lisfranc Injury, Tarsometatarsal Joint Injury, Tarsometatarsal Joint Complex Injury, Lisfranc Dislocation
- See Also
- Epidemiology
- Accounts for 0.1 to 0.4% of all Fracture dislocations
- Pathophysiology
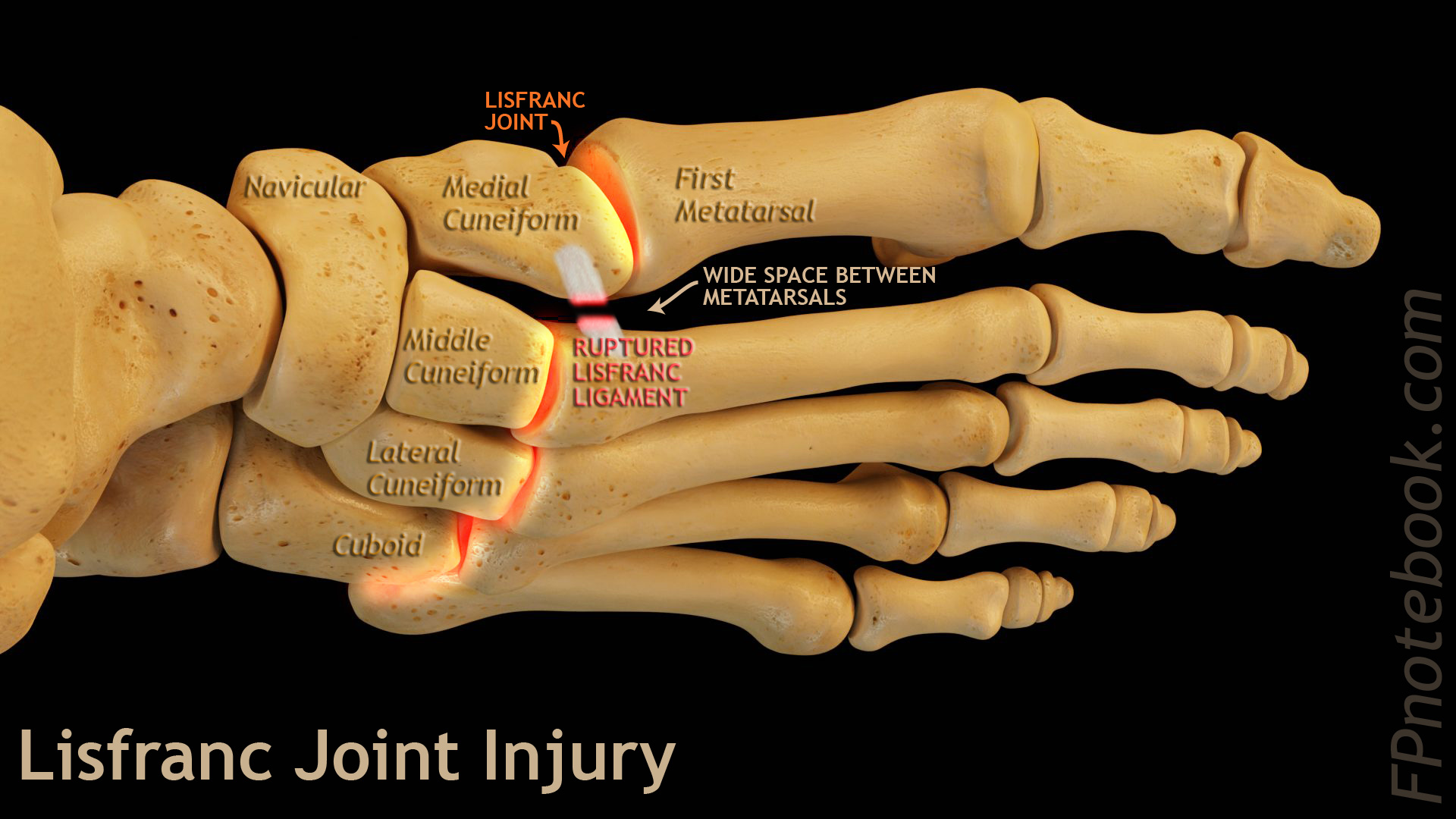
- Lisfranc Joint: Tarsometatarsal articulation of foot (between midfoot and forefoot)
- First three Metatarsal articulate with the Cuneiform Bone
- Fourth and Fifth Metatarsals articulate with the Cuboid Bone
- Lisfranc ligament
- Attaches second Metatarsal base to medial Cuneiform (plantar surface stronger, dorsum weaker)
- Key to midfoot stability (susceptible to Trauma)
- Keystone wedging of base of second Metatarsal
- Articulates with Second Cuneiform
- Straddled by first and Third Cuneiform
- Lisfranc joint transfers force from mid to forefoot
- Critical to plantar flexion and dorsiflexion
- Lisfranc is the central keystone support for the two foot arches (longitudinal and transverse)
- Lisfranc helps stabilize the foot in standing and gait
- Lisfranc Injury undermines arch and midfoot stability
- Images
- Precautions
- Lisfranc joint injury may be subtle and is initially missed or misdiagnosed in 20% of cases
- Mechanism
- Foot in plantar flexion, undergoes rotation or compression, then axial loading
- Displaces second Metatarsal dorsally
- Types of injuries
- High Energy Direct Injury
- Motor Vehicle Accident
- Heavy equipment related crush injury
- Low Energy Indirect Injury
- Sports (e.g. football, dance)
- Missed step on staircase or curb, and falls forward onto plantar-flexed foot
- High Energy Direct Injury
- Causes
- Lateral Ankle Sprain
- High energy injury
- Motor Vehicle Accident
- Fall from high height
- Symptoms
- Persist >5 days after injury
- Midfoot swelling
- Difficult weight bearing
- Signs
- Neurovascular exam
- High mechanism injury
- Risk of dorsalis pedis artery branch injury (first web space) and foot Compartment Syndrome
- Risk for deep peroneal nerve injury
- Ecchymosis at plantar surface of midfoot (pathognomonic)
- Difficult weight bearing while on tiptoes
- Tenderness at tarsometatarsal joint
- Pain on squeezing the midfoot between the examiners fingers (medial and lateral)
- Piano key test
- Stabilize the midfoot
- Palpate the head of each Metatarsal for pain and instability
- Types
- Homolateral Lisfranc Dislocation
- Lateral Metatarsal displacement
- Divergent Lisfranc Dislocation
- Medial Metatarsal displacement of first Metatarsal Bone
- Lateral Metatarsal displacement of other Metatarsal Bones
- Isolated Lisfranc Dislocation
- Dorsal dislocation of 1 or 2 Metatarsal Bones
- Imaging
- XRay Foot
- Consider Foot CT or Foot MRI if XRay not diagnostic
- Foot CT identifies 60% more Metatarsal Fractures and twice as many Tarsal Fractures as XRay
- Foot CT or Foot MRI is commonly needed for diagnosis (but start with xray)
- Also consider Foot CT if the patient cannot bear weight for a Lateral XRay
- Foot MRI is preferred to evaluate for ligamentous sprain without bony injury
- Have a low threshold for avanced imaging (or non-weight bearing, immobilization and close specialty follow-up)
- Efficacy
- Initial False Negative Rate is high (20-50%)
- Weight bearing images are critical for accurate diagnosis
- Views (consider comparison views with opposite foot)
- Anteroposterior Foot XRay
- Widening of space (diastasis) between first and second Metatarsal heads
- Wide if >=2.7 mm
- Widening of space (diastasis) >2 mm between second Metatarsal base and medial Cuneiform
- Malalignment or step-off at medial borders of second/middle Cuneiform and second Metatarsal
- Draw a line along the second Metatarsal medial shaft and base AND the medial middle Cuneiform
- Draw a line along the fourth Metatarsal medial shaft and base AND the medial Cuboid
- Avulsed Metatarsal base of Cuneiform Bone fragments (fleck sign)
- Proximal second metarsal is most common associated Fracture
- Widening of space (diastasis) between first and second Metatarsal heads
- Oblique XRay View
- Lateral borders of third Metatarsal and lateral Cuneiform malaligned
- Medial borders of fourth Metatarsal and Cuboid malaligned
- Lateral Foot XRay (weight bearing): Step-off on dorsal foot surface
- Loss of arch height (Stage III injury)
- Proximal first or second Metatarsal displaced dorsally or upward
- Middle Cuneiform top below Metatarsal top
- Cuboid not aligned with Metatarsals
- Avulsion Fractures suggestive of Lisfranc Injury
- Management
- Conservative Management
- Orthopedic or podiatry Consultation is recommended for all suspected Lisfranc injuries
- Unstable injuries should receive emergent Consultation for surgical intervention
- Stable Fractures or dislocations may be splinted and followed up in orthopedics in 1-2 weeks
- Other referral indications (see surgery indications below)
- Lisfranc joint displacement >2 mm
- Joint Instability
- Reduction Indications (Regional Anesthesia or Procedural Sedation)
- Reduce significant acute, closed dorsal dislocations in the emergency department
- Immobilization
- Splint patients and avoid weight bearing if any suspicion of Lisfranc Injury
- Start: Short-leg Non-weight bearing cast or boot for first 4-6 weeks
- Next: Short-leg weight bearing cast or boot for another 2 to 4 weeks
- Rehabilitation after cast or boot removal
- Expect 6-12 months before resuming full activity after a significant lisfranc joint injury
- Reassess 2 weeks after starting rehabilitation
- Repeat weight bearing XRays to assess for instability
- Management
- Surgery
- Indications
- Displacement greater than 2 mm
- Unstable Fracture dislocations with instability
- Most Lisfranc injuries evident on imaging are unstable
- Timing
- Best performed within first 24 hours of injury
- Some prefer to wait 7-10 days for less swelling
- Efficacy
- Best functional outcomes are with surgery (unless Lisfranc Injury is stable)
- Complications
- Post-Traumatic arthrosis and Chronic Pain
- Midfoot and Gait Instability (due to longitudinal and transverse arch disruption)
- Foot Compartment Syndrome
- Acute complication from high energy injury with significant bony displacement
- Disrupts the dorsalis pedis branch that runs between the first and second Metatarsals
- Results in significant soft tissue swelling
- Prognosis
- High risk of morbidity with Disability related to ambulation
- References
- Young (2022) Crit Dec Emerg Med 36(8): 16-7
- Gaskin and Denq (2020) Crit Dec Emerg Med 34(4): 16-7
- Feden and Kiel (2017) Crit Dec Emerg Med 31(11): 3-10
- Burroughs (1998) Am Fam Physician 58(1): 118-24 [PubMed]
- Grewel (2020) Foot 45:101719 [PubMed]
- Riveros (2025) Crit Dec Emerg Med 39(11): 24-5 [PubMed]
- Silver (2024) Am Fam Physician 109(2): 119-29 [PubMed]