Peritonsillar Abscess Drainage, Peritonsillar Abscess Needle Aspiration
- See Also
- Indications
-
Peritonsillar Abscess
- Alternatives: Incision and Drainage or Tonsillectomy by ENT
- Precautions
- Carotid Artery runs 2 cm posterolateral to the Tonsillar Pillar
- Do not insert aspiration needle more than 8 mm
- Management
- Primary Anesthetic
- Step 1: Spray with Topical Anesthetic
- Lidocaine 1% with Epinephrine via MADD atomizer (author preference) OR
- Benzalkonium 0.5% spray (Cetacaine)
- Step 2: Gargle 1-2% Lidocaine with Epinephrine
- Alternative Anesthetic
- Sphenopalatine block
- Local Anesthetic injection
- Inject into mucosa overlying region of fluctuance using 25-27 g 1.5 inch needle OR
- Inject Lidocaine 1% with Epinephrine into mucosa with aspiration needle and then aspirate
- Technique
- Preparation
- Be prepared for airway emergency (e.g. bleeding)
- Suction with Yanker tip
- Light source: Direct Laryngoscope with curved blade (Macintosh Blade)
- Position overlying the Tongue, lighting the posterior pharynx, but not so deep as to trigger a Gag Reflex
- Patient as assistant (if sufficiently calm)
- Patient may hold shallowly placed Laryngoscope Blade in place with one of their hands
- Patient may hold the suction catheter with their opposite hand
- Patient positioning
- Patients sits forward, at eye level to examiner
-
Ultrasound with endocavitary probe
- Helps to guide needle towards largest abscess pocket
- Trismus may limit use
- References
- Lin in Herbert (2014) EM:Rap 14(4): 5-7
- Technique
- Needle Aspiration
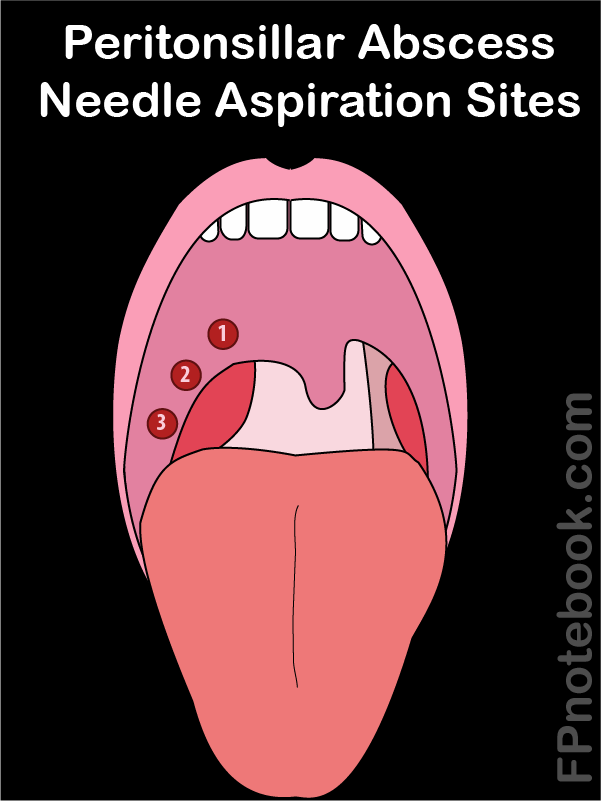
- Images
- Retract Tongue
- Tongue blade or
- Laryngoscope Blade (consider having patient hold this, see above)
- Needle 18 gauge on 3 cc syringe
- Consider longer needle (e.g. spinal needle) obstructs view less
- Smaller syringe requires less force to withdraw plunger
- Use a needle guard
- Prevents entrance into Carotid Artery
- Cut off distal 0.5 to 1 cm of plastic needle cover
- Needle should protrude only 0.5 to 1 cm beyond guard
- Tape needle cover to syringe to secure
- Avoid lateral margin of Tonsil
- Carotid Artery is 2 to 2.5 cm posterolateral to Tonsil
- Keep needle in Sagittal Plane
- Aspirate most fluctuant area
- Superior pole of Tonsil most commonly affected
- Aspirate peritonsillar space (medial Soft Palate)
- Tonsil itself is not aspirated
- Failed aspiration
- Move the needle inferolaterally along the Soft Palate and reattempt aspiration up to twice more
- Exercise caution, as carotid puncture increases in risk with inferior needle placement
- Complications
- Patient aspiration of pus or blood
- Hemorrhage from puncture of Carotid Artery
- Failed Needle Aspiration
- Peritonsillar Abscess recurrence (10%)
- References
- Warrington (2017) Crit Dec Emerg Med 31(4): 17