Extensor Tendon Injury at the DIP Joint, DIP Extensor Tendon Avulsion, Mallet Finger, Mallet Fracture, Drop Finger, Baseball Finger
- See Also
- Epidemiology
- Mallet Finger is the most common closed finger Tendon Injury
- Mechanism
- Forced flexion of extended distal interphalangeal joint
- Ball strikes fingertip on catching a ball
-
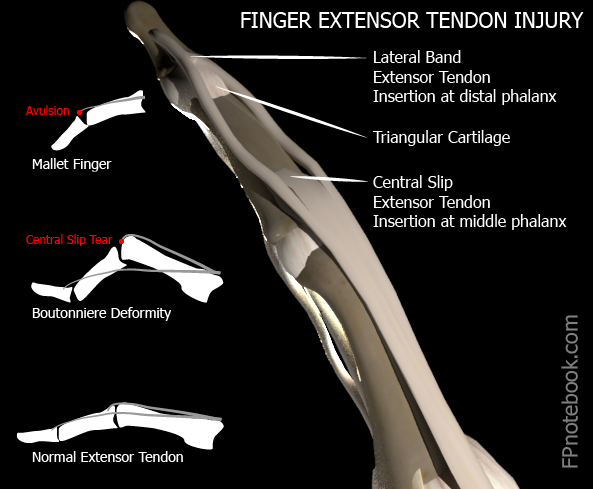
Trauma at DIP joint results:
- Avulsion of distal phalanx (Bony Mallet) as extensor tendon tears away bony insertion or
- Pure extensor tendon rupture (Tendinous Mallet)
- Tendon stretched or torn (partially or completely)
- Images
- Symptoms
- Pain, Bruising and swelling at dorsal DIP joint
- Signs
- DIP joint with flexion deformity at rest
- Intact flexor tendon unopposed by the ruptured extensor tendon
- Isolate the DIP joint to test active extension
- Variable loss of active finger DIP extension
- Confirm extension weakness due to extensor tendon
- Central slip at PIP joint can also extend DIP
- Associated Conditions
- Volar subluxation of distal phalanx with bony mallet
- Imaging
- XRay of digit (esp. lateral)
- Management
- Splinting
-
General
- Splints are equally effective: Aluminum, Stack, Ring
- Stack splint is most commonly used
- Splints are as effective as surgical repair
- May participate in sports with splinted DIP
- Splints are equally effective: Aluminum, Stack, Ring
- Technique
- May use prefabricated splint instead
- Measure and cut the splint to extend from fingertip to the middle phalanx
- Should only immobilize the DIP joint (not the PIP joint)
- Smooth sharp edges
- Mold the splint to keep the DIP joint in slight hyperextension (5-10 degrees)
- Splint may be applied to either the dorsal or volar surface (author prefers volar surface)
- Tape the splint in place
- Precautions
- See Orthopedic referral indications below
- Splint should not reduce range of motion of PIP
- Splinting must be continuous for entire period (DIP must remain in extension)
- Splinting time (6-8 weeks) restarts if the finger falls back into flexion
- Delayed presentation (e.g. month old injury) requires a longer period of Splinting
- Risk of skin necrosis with Splinting
- Avoid pressure to dorsum of DIP
- Avoid hyperextension of DIP joint
- Skin will blanch if DIP hyperextended
- Assessment
- Post-reduction XRay to confirm proper alignment
- Protocol
- First 6-8 weeks
- Splint finger in neutral extension for 6-8 weeks
- Splinting must be continuous without fail
- Twenty four hours per day
- Every day for 6-8 weeks
- Hold extension when changing splint
- Support distal phalanx against flat surface
- Ask for assistance when changing splint
- Allow skin to air for 10 minutes at splint change
- Reduces maceration at splint
- Restart 8 week Splinting period if finger flexes
- Next 3-6 weeks
- Splint finger in extension only at night
- First 6-8 weeks
- Management
- Orthopedic Referral Indications (see prognosis below)
- Joint incongruent
- Inability to passively extend DIP joint
- Suggests bone or soft tissue entrapment
- Fracture involves >30% of joint space
- Fragment displaced >2mm
- Open Growth Plate
- Bony avulsion >1/3 of distal phalanx
- Volar subluxation of distal phalanx
- Management
- Follow up
- Re-examine every two weeks until healed
- XRay every two weeks if bony avulsion
- Management
- Anticipatory Guidance
- Warn that patient that outcome will not be perfect
- Prognosis
- Outcomes are similar for conservative therapy versus surgical management (regardless of referral indications above)
- Complications
- Chronic loss of full distal phalanx extension
- References
- Brandenburg (1996) Consultant p.331-340
- Calmbach (1996) Lecture in Minneapolis
- Dvorak (1996) Lecture in Minneapolis
- Lillegard (1996) Lecture in Minneapolis
- Warrington (2023) Crit Dec Emerg Med 37(3): 22
- Childress (2022) Am Fam Physician 105(6): 631-9 [PubMed]
- Hilgefort (2025) Am Fam Physician 112(1): 47-54 [PubMed]
- Leggit (2006) Am Fam Physician 73(5):810-6 [PubMed]
- Simpson (2001) J Hand Surg 26:32-3 [PubMed]
- Wang (2001) Am Fam Physician 63(10):1961-66 [PubMed]