Dorsal PIP Dislocation, Dorsal Proximal Interphalangeal Joint Dislocation, Finger Dislocation at Dorsal PIP Joint
- See Also
- Epidemiology
- Most common finger dislocation
- Mechanism
- Occurs due to blow to end of finger with hyperextension
- Exam
- Signs
- Finger deformity at middle phalanx dorsum
- Volar plate tenderness to palpation
- Splinting for 4 to 6 weeks if Volar Plate Injury suspected
- Complications
- Proximal, Middle Phalanx Fracture
- Volar plate Fracture is commonly present
- Surgery may be needed if involves >30-40% of joint surface
- Risk of PIP flexion deformity if not repaired
- Imaging
- Post-Reduction Evaluation
- Subluxation or PIP joint instability
- Volar plate Fracture
- Management
- Reduction in clinical setting
- See reduction on the sideline below
-
Local Anesthesia if >1 hour since dislocation
- Digital Nerve Block or
- Joint block
- Maneuver (usually effective)
- Hand 1: Hold proximal phalanx to stabilize
- Hand 2: Hold middle phalanx for traction/pressure
- Apply distal traction
- Volar directed pressure at middle phalanx base
- Deformity obviously reduces with maneuver
- Additional measures if refractory to above
- Hyperextend distal part and retry maneuver above
- Hand 1 (proximal) can apply gentle pressure at base of dislocated phalanx, pushing the phalanx distally
- Difficult reduction suggests interposed tissue
- Management
- Reduction on sideline
- Reduce with maneuver above
- May forego finger XRay prior to reduction
- Digital Block not needed if <1 hour from injury
- Criteria for completing game
- Affected finger splinted with buddy tape and
- Straight-forward reduction and
- Stable joint assessment (see above)
- Follow-up in clinic
- Requires clinical assessment and
- Finger XRay
- Management
- Post-reduction
- Joint evaluation post-reduction
- Imaging as above
- Assess joint range of motion
- Assess collateral ligaments with PIP flexed
- Assess volar plate by palpation and hyperextending joint
- Extend flexed pip against resistance
- Inability suggests central slip disruption
- Refer abnormal exams to orthopedics (Boutonniere risk)
- Management
- Immbolize for 4 to 6 weeks if Volar Plate Injury suspected
- Immobilize for 3 weeks
- First: Splint 1-2 weeks

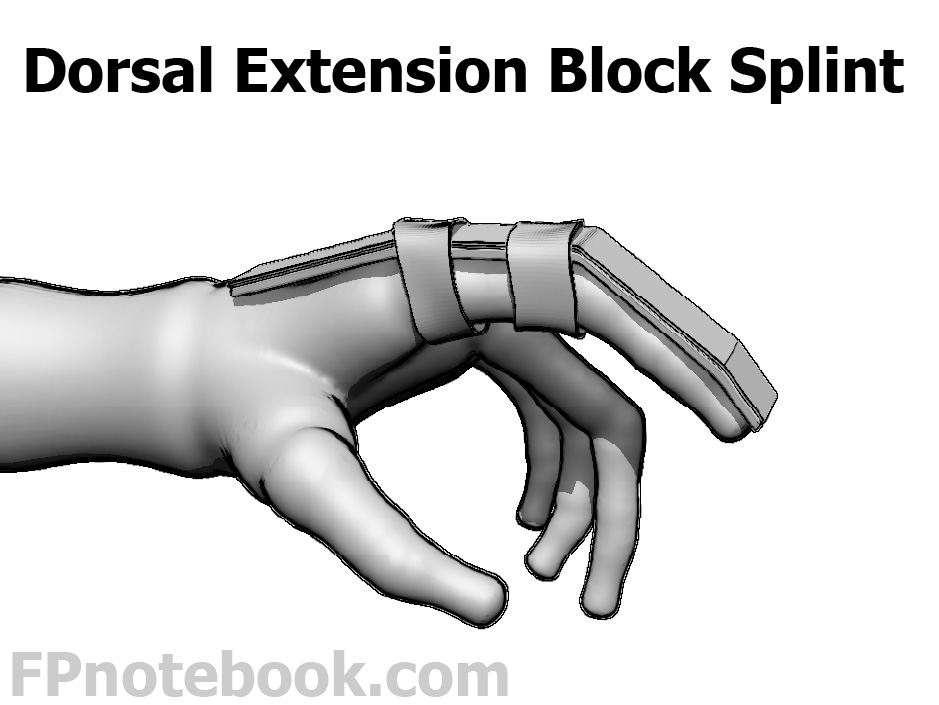
- Dorsal extension block splint in 20-30 degrees of flexion at PIP joint
- Aluminum Foam splint affixed to dorsal finger
- Splint extends from distal tip to proximal Metacarpals
- Splint taped to finger at the proximal phalanx and distal Metacarpal
- DIP and PIP joints are allowed to flex freely, but splint prevents extension of finger
- Next: Buddy tape finger for additional 1 to 2 weeks
- First: Splint 1-2 weeks
- Early range of motion and strengthening
- Follow-up
- Repeat XRay and evaluation in one week
- Orthopedic referral indications
- Unable to relocate joint despite above maneuvers
- Avulsion Fracture involving more than 30-40% of the interphalangeal joint surface
- Incomplete extension following reduction
- Complications
- Chronic Pain
- Degenerative joint changes at the dislocated joint
- Functional loss (loss of range of motion)