CT Head, Head CT, CT Brain, Contrast Staining on Non-Contrast Head CT, Head CAT Scan
- See Also
- Indications
-
Cerebrovascular Accident
- Differentiate Hemorrhagic CVA from Ischemic CVA
- More sensitive than LP for Intracranial Hemorrhage
-
Test Sensitivity diminishes from time of Hemorrhagic CVA
- Test Sensitivity 95-100% at 12 hours from onset
- Test Sensitivity 50% at 7 days from onset
- Hemorrhagic CVA is not detectable on CT Head at 2-3 weeks from onset
- Suarez (2006) N Engl J Med 354(4): 387-96 [PubMed]
-
Brain Tumors (larger than 2-4 mm)
- Enhanced with iodinated Contrast Material
-
Hydrocephalus
- Temporal horn of the Lateral Ventricle dilates (axial width >=5 mm) early in Hydrocephalus
- Appear rounded as Hydrocephalus develops (contrast with their normal curved-slit appearance)
-
Third Ventricle appears O-Shaped when dilated from downstream CSF obstruction
- Third Ventricle is normally has a more slit-like appearance
- Temporal horn of the Lateral Ventricle dilates (axial width >=5 mm) early in Hydrocephalus
-
Intracranial Bleeding
- Epidural Hematoma
- Subdural Hematoma
- Intraparenchymal Hemorrhage
- Subarachnoid Hemorrhage (Thunderclap Headache)
- Evaluation of Traumatic Head Injury
- CT Head in every Severe Head Injury
- CT Head in every Moderate Head Injury
- See Head Injury CT Indications
- See Head Injury CT Indications in Children
- Interpretation
- General
- See CT Scan Window Width
- Describes CT Windows for Brain Window or Subdural Window
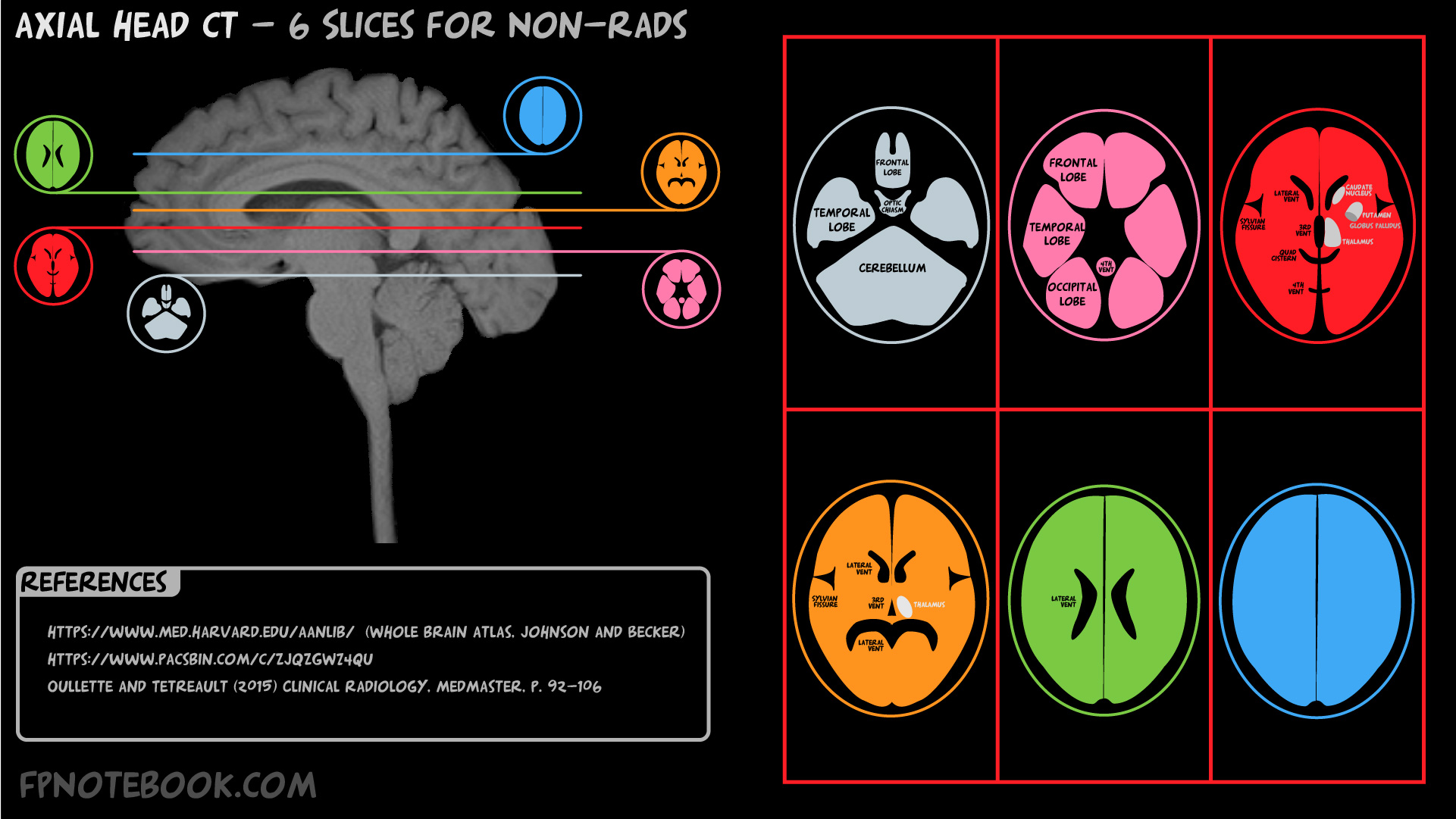
- Scout View (lateral head with 6 parallel lines delineating key slices)
- Overview
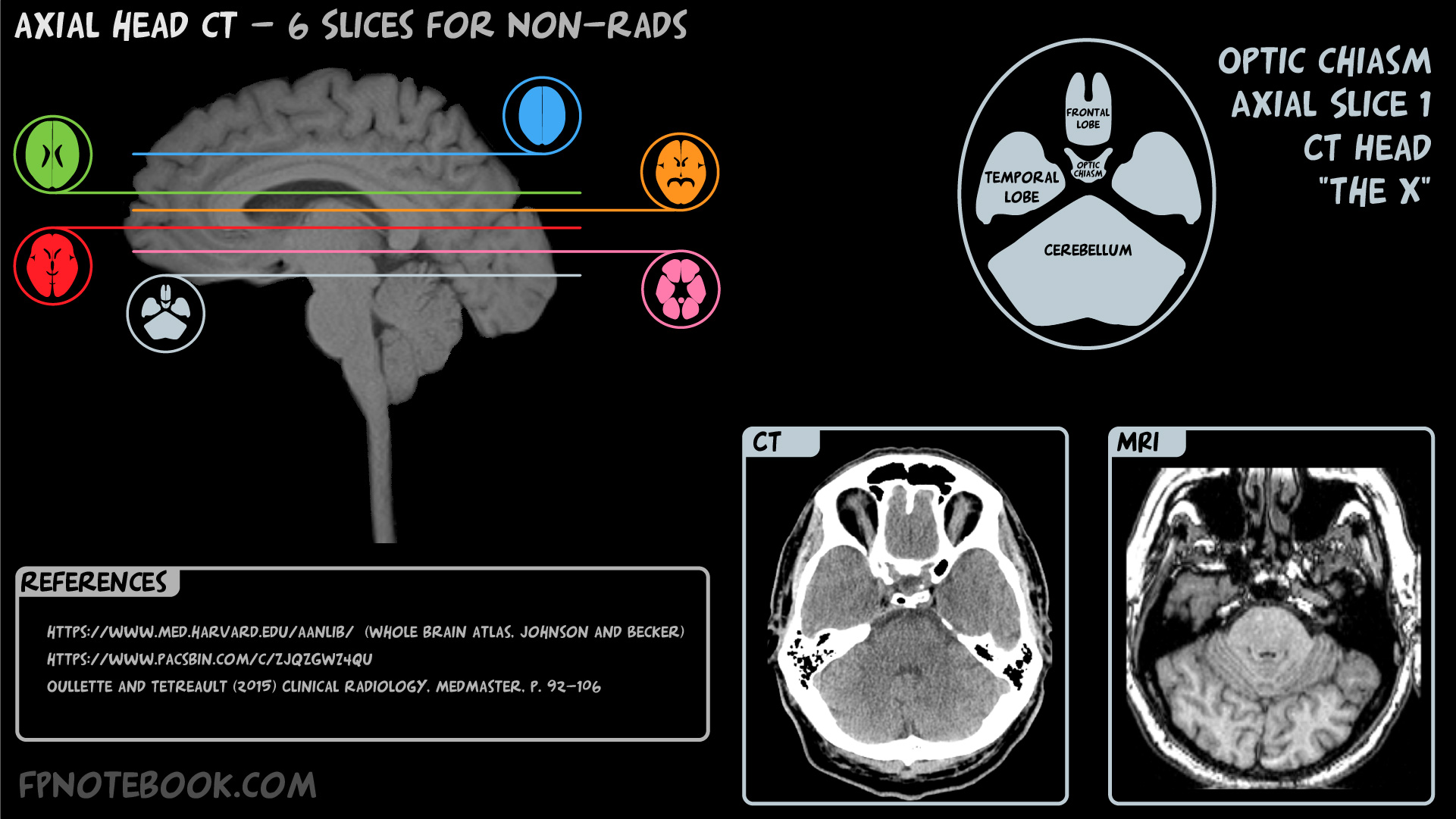
- Skull Base

- Appears as an X dividing key structures
- Frontal Lobe and Frontal Sinuses
- Temporal Lobes (left and right)
- Mastoid Air Cells (bilateral appearance confirms symmetry of the imaging)
- Basilar Artery
- Fourth Ventricle
- Cerebellum
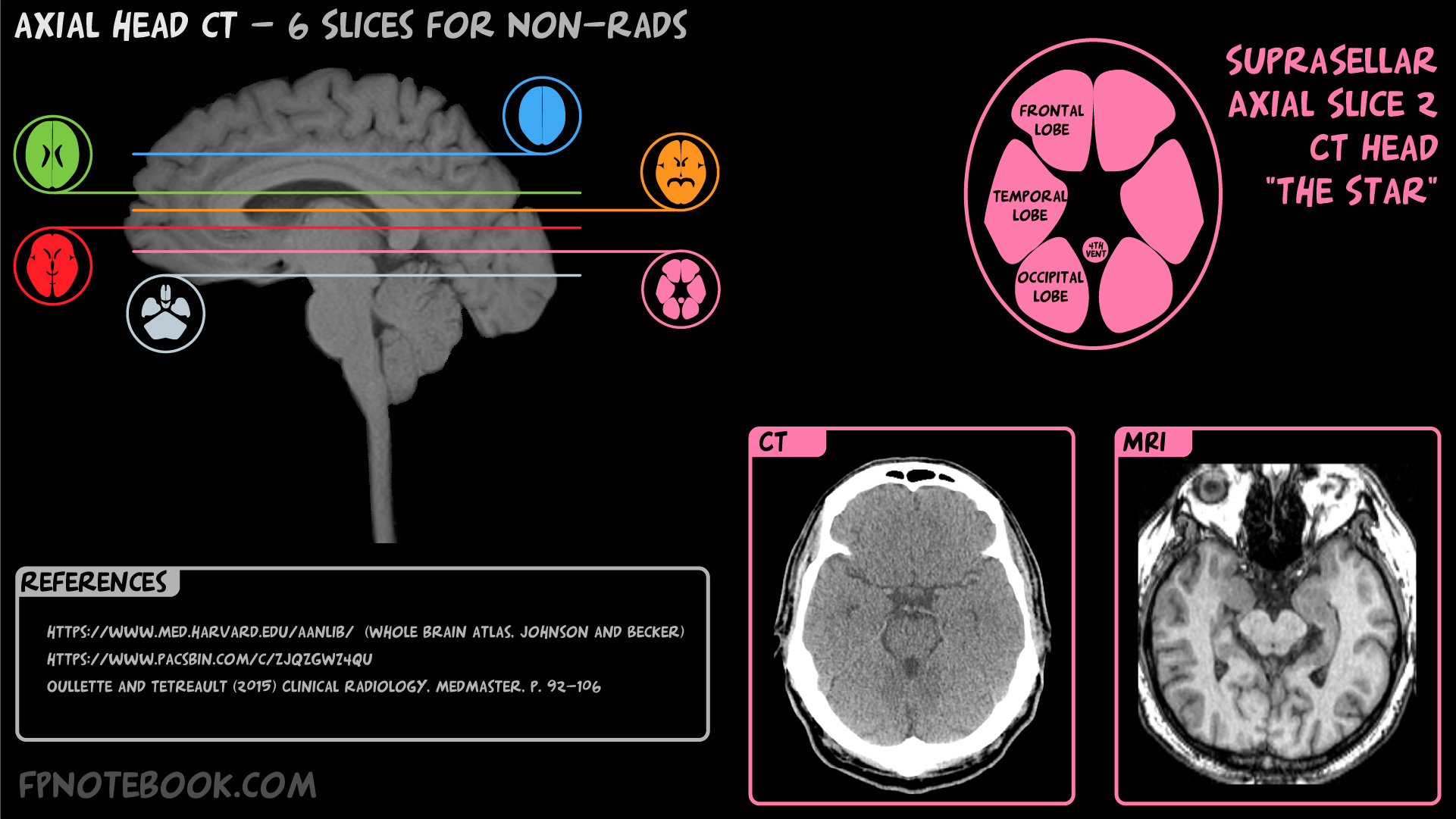
- Basic Slice 2

- Appears as a central 5-sided star (suprasellar cistern, superior to the sella turcica)
- Frontal Lobes
- Temporal Lobes
- Circle or Willis
- Brainstem (at Midbrain or Pons level)
- Cerebellum
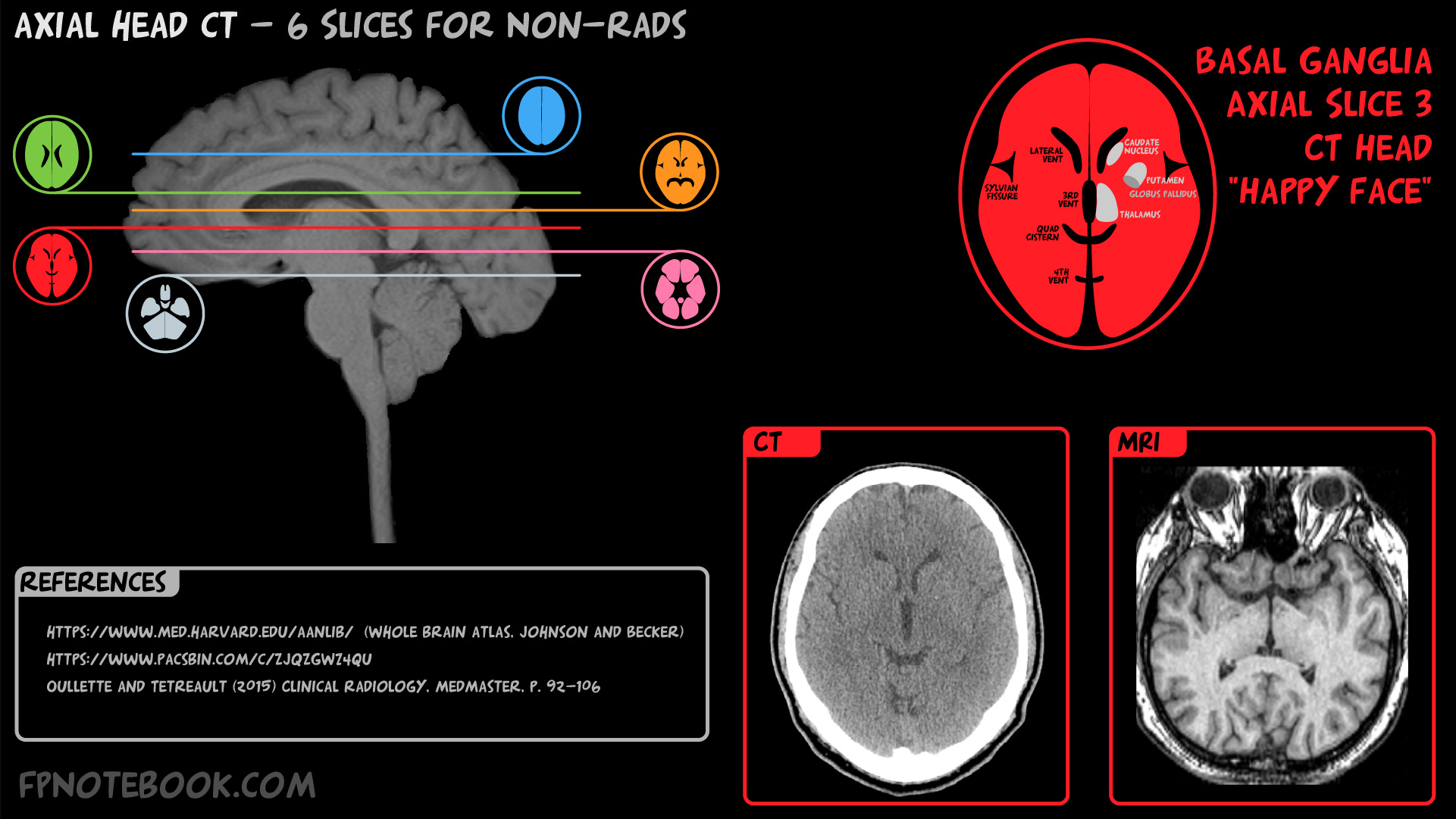
- Basic Slice 3

- Appears as a smiling face
- Eyes = Lateral Ventricles
- Mouth = quadrigeminal cistern
- Frontal Lobes
- Putamen
- Parietal Lobes
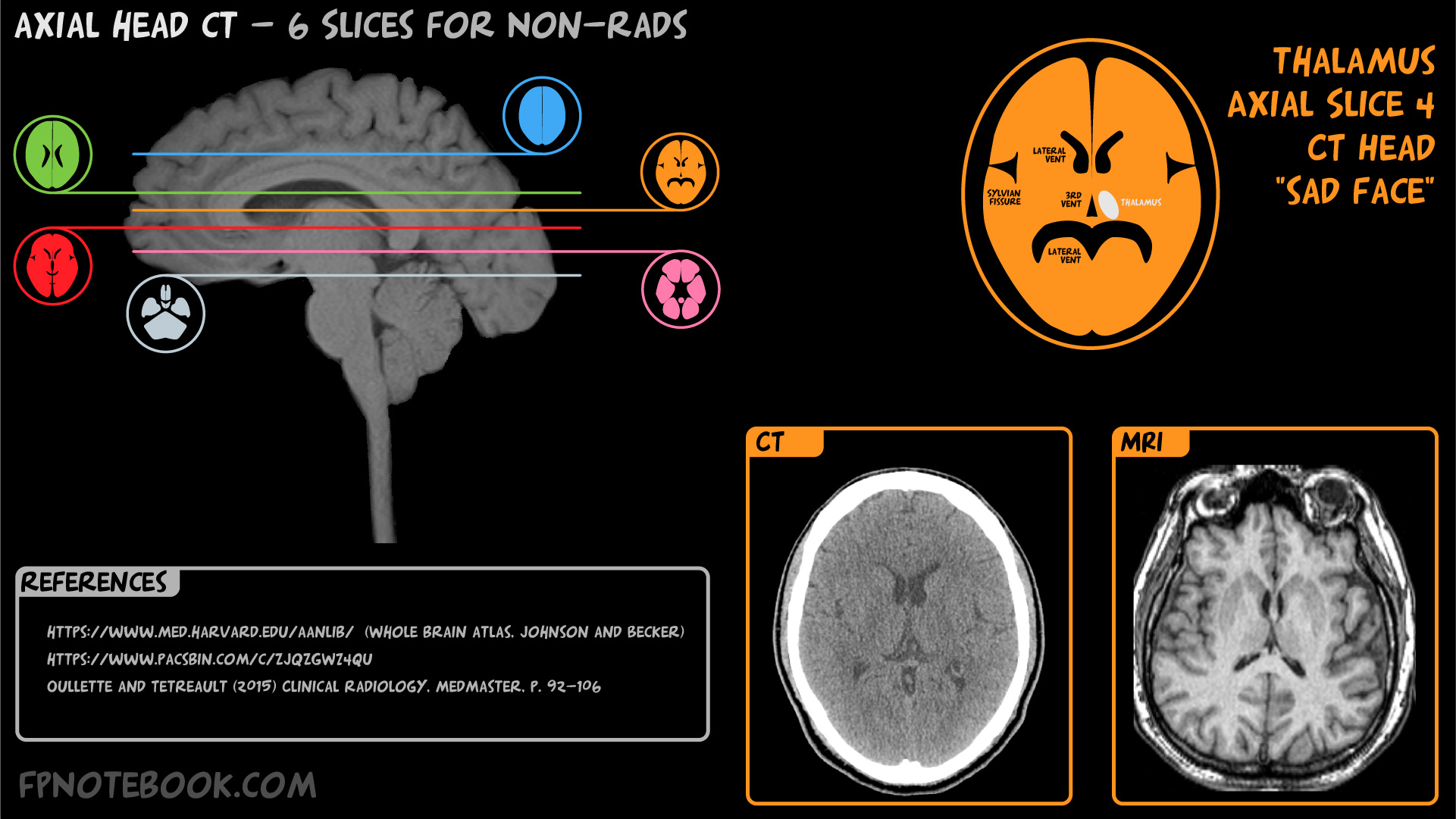
- Basic Slice 4

- Appears as a frowning face
- Eyes = Lateral Ventricles
- Mouth = Lateral Ventricles
- Nose = Third Ventricle
- Frontal Lobes
- Thalamus (to either side of Third Ventricle)
- Internal Capsule
- Parietal Lobes
- Calcified structures
- Pineal Gland (central, near Third Ventricle)
- Choroid plexus (in posterior Lateral Ventricles)
- Colloid cysts may also appear in Third Ventricle (may cause Obstructive Hydrocephalus)
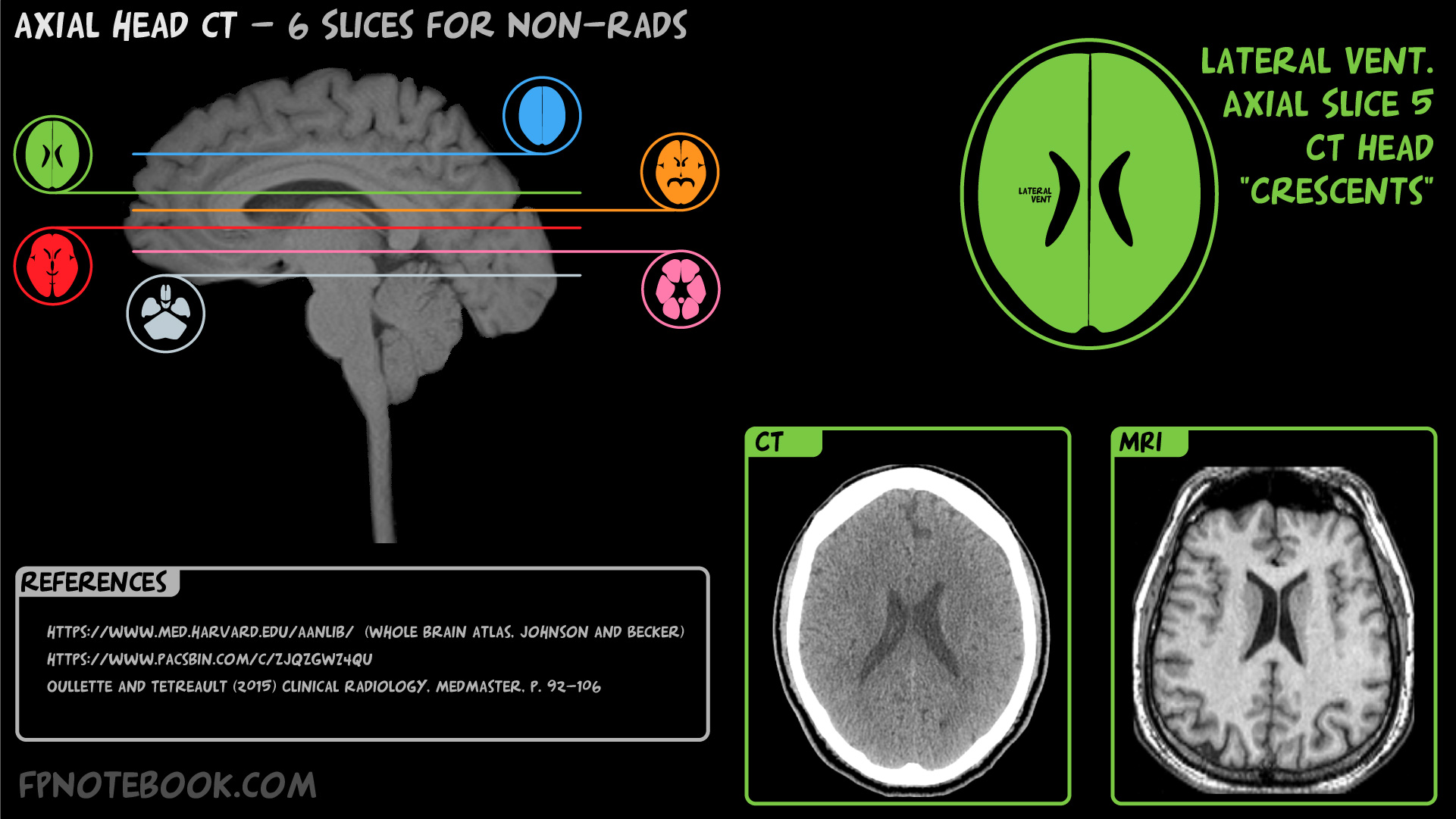
- Basic Slice 5 (appears as 2 bananas, concave laterally = Lateral Ventricles)
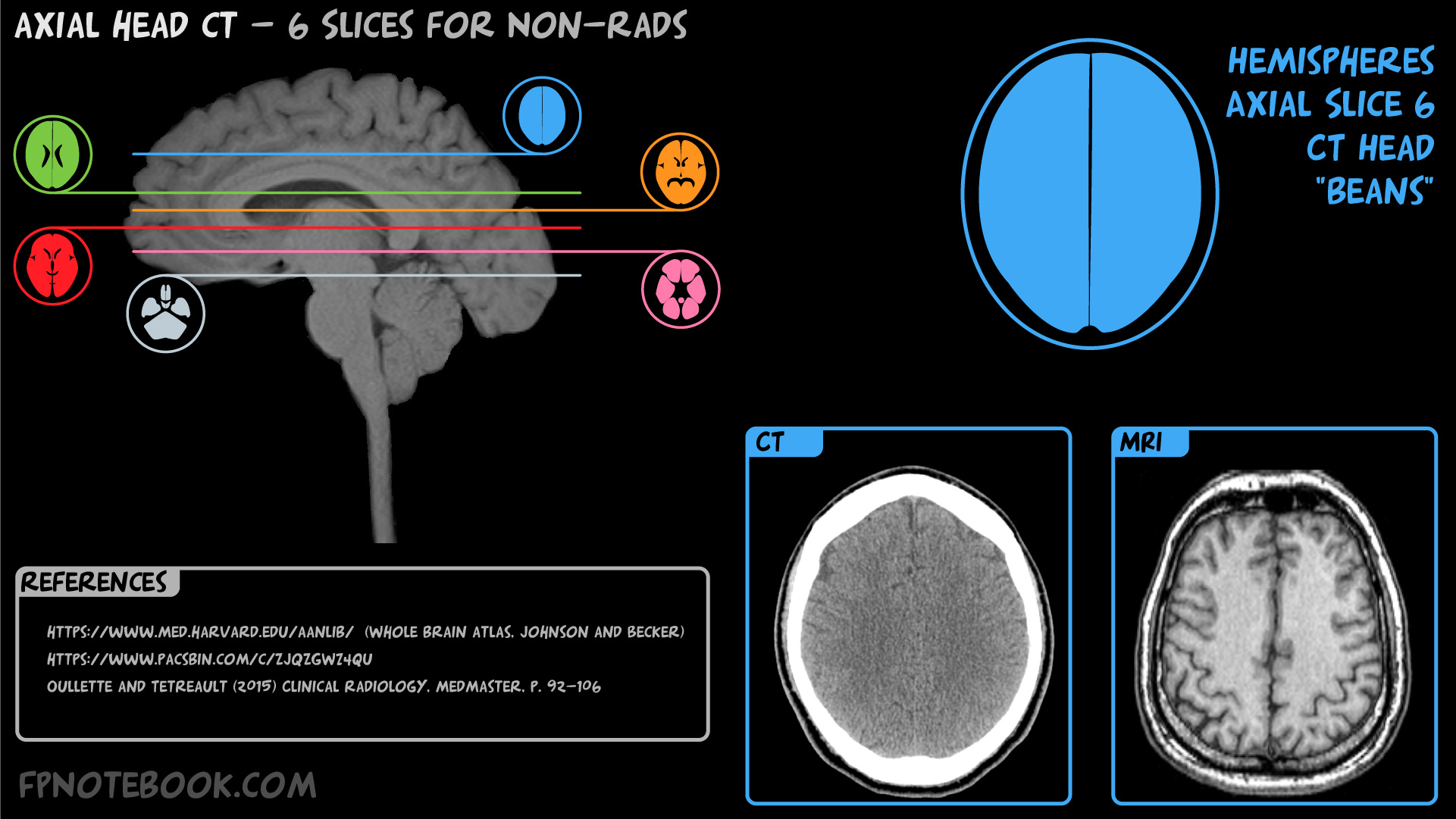
- Basic Slice 6 (appears as a Coffee bean with 2 hemispheres with a central split)
- Overview
- Interpretation
- Systematic Approach Mnemonics
- ABCS2
- A: Alignment and Abnormalities-Major
- Symmetry between sides using small well defined structures (e.g. eye lenses, masotid air cells)
- Basic slices (see above) are oriented correctly
- B: Blood and Brain
- C: CSF and Cisterns
- S: Skull and Subdural Windows
- A: Alignment and Abnormalities-Major
- "Blood Can Be Very Bad"
- B: Blood
- Background
- Recent Hemorrhage will appear bright white
- Darkens as it ages (isodense to brain at week 1-3, isodense to CSF at >3 weeks)
- Cerebral sulci flatten and become less apparent with Hemorrhage or brain edema
- Intraventricular Hemorrhage (e.g. SAH) may be best seen at the occipital horns of the Lateral Ventricles
- Use subdural windows (or lower contrast/brightness) to differentiate acute blood from bone (similar HU densities)
- Recent Hemorrhage will appear bright white
- Hemorrhages
- Epidural Hematoma (biconvex lens appearance)
- Subdural Hematoma (crescent moon appearance, cross Suture lines but not the falx or tentorium)
- Cerebral Intraparenchymal Hemorrhage or Traumatic Intracerebral Hemorrhage
- Subarachnoid Hemorrhage (SAH) or Traumatic Subarachnoid Hemorrhage
- Other findings
- Dense Vessel sign
- Bright white appearance of clotted vessel (e.g. MCA)
- Venous sinus thrombosis
- Venous clot (bright white) may be seen in some cases on non-enhanced CT
- If suspected, obtain CTV or MRV
- Dense Vessel sign
- Background
- C: Cisterns
- B: Brain
- Cerebral infarcts (black)
- Cerebral masses (or mass effect with midline shift)
- Edema
- Grey-white differentiation
- Homogeneous appearance is abnormal (e.g. anoxic brain injury, acute CVA)
- Zoom out of image (or move back away from monitor) to see regions of different attenuation
- V: Ventricles
- Abnormally large (Hydrocephalus)
- Abnormally small (slit-like ventricles)
- Sulcus effacement (lose contours, compressed against skull, when ICP increased)
- Herniation
- Subfalcine Herniation (midline shift, most common)
- Transtentorial Herniation (Uncal Herniation)
- Cerebellar Herniation (Tonsillar Herniation, least common)
- B: Bone (using bone windows)
- Skull Fracture
- Cancer (e.g. metastases, Multiple Myeloma)
- Pneumocephalus (more evident with bone windows)
- B: Blood
- Interpretation
- Hemorrhage
-
Hemorrhage appearance on CT changes with time
- Acute Hemorrhage: Hyperdense (light, white)
- Whiter than brain matter
- Subacute Hemorrhage: Isodense
- Similar density to brain matter and may be missed
- Chronic Hemorrhage: Hypodense (dark)
- Darker than brain matter
- Old Subdural Hematoma may appear as a hygroma
- Acute Hemorrhage: Hyperdense (light, white)
-
Hemorrhage mimics: Contrast Staining
- Contrast staining refers to contrast deposition in extravascular brain parenchyma after IV contrast
- Non-contrast CT Head demonstrates a bright appearance similar to CNS Hemorrhage appearance
- Contrast staining occurs with transient increased blood brain permeability
- Intracranial neoplasm
- Ischemic CVA
- Intra-arterial clot extraction
- Contrast staining differs from CNS Hemorrhage in several ways
- Contrast staining typically resolves more quickly than Hemorrhage (24-48 hours)
- Contrast staining remains confined to the original lesion (while Hemorrhage extends)
- Contrast staining typically has attenuation <50 HU following endovascular thrombectomy
- Additional Imaging can also help distinguish between contrast staining and Hemorrhage
- Serial CT Head (repeated in 6 hours, traditional method)
- Dual energy CT
- MRI with susceptibility weighted imaging
- References
- Broder (2025) Crit Dec Emerg Med 39(10): 26-8
- Contrast staining refers to contrast deposition in extravascular brain parenchyma after IV contrast
- References
- Ouellette and Tetreault (2015) Clinical Radiology, Medmaster, Miami, p. 92-106
- Broder (2024) Crit Dec Emerg Med 38(7): 22-3
- Broder (2021) Crit Dec Emerg Med 35(5): 10-1
- Haydel (2000) N Engl J Med 343:100-5 [PubMed]