Ultrasound in Abdominal Aortic Aneurysm, Ultrasonography of Abdominal Aortic Aneurysm, Ultrasound of AAA, Abdominal Aorta Ultrasound, Ultrasound of Abdominal Aorta
- Indications
- Cases in which Ultrasound is AAA imaging modality of choice
- Screening for Abdominal Aortic Aneurysm
- See Abdominal Aortic Aneurysm for screening indications
- Monitoring Abdominal Aortic Aneurysm rate of change
- Screening for Abdominal Aortic Aneurysm
- Other Indications
- See RUSH Exam
- Emergent Bedside Ultrasound in suspected AAA rupture (combine with FAST Exam)
- Efficacy
- Efficacy when performed by Radiology Ultrasonographer
- Highly accurate even when performed by Emergency Physicians
- Test Sensitivity: ~100% (in practice, likely approaches 94% as study above)
- Test Specificity: 98%
- Accurate to within 0.3 cm in sizing aneurysm (compared with CT)
- Tayal (2003) Acad Emerg Med 10(8): 867-71 [PubMed]
- Good efficacy has been found for medical students after only 3 hours of training
- Primary care physicians were trained 25 hours using hand-held Ultrasound, and could perform accurate exam in 4 minutes
- Contrast with with physical exam whose accuracy is notoriously poor until AAA reaches a size that is at high risk for rupture
- Limitations
- Does not define periaortic Vascular Anatomy
- Reduced image quality in some patients
- Obese patients
- Increased intestinal gas
- Precautions
- Apply firm pressure to push bowel gas out of the way (especially in obese patients)
- Err on the side of overestimation of AAA size due to difficulties in estimating size of clot
- Consider color doppler to assist in highlighting aorta
- But probe most be directed with the flow or against the flow (not perpendicular)
- Imaging
- Approach
- Transducer
-
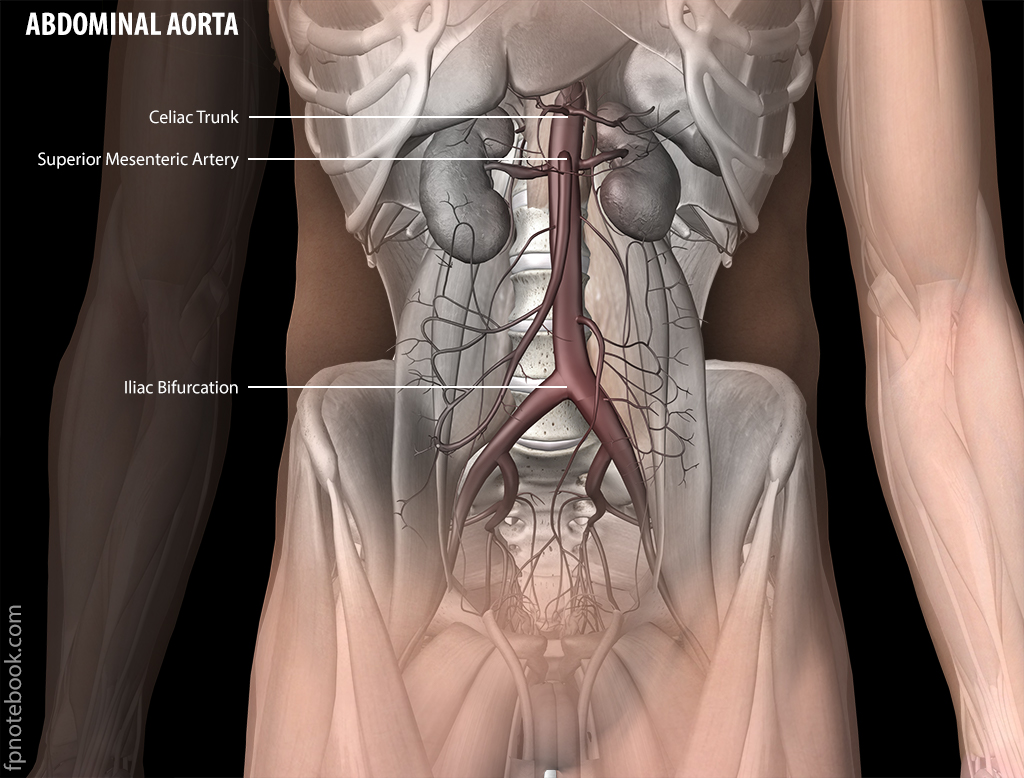
General landmarks
- Start in upper Abdomen at the epigastrium, and slide probe inferiorly
- Liver may be used as acoustic window for proximal abdominal aorta
- Vena cava will be to the patient's right side of the aorta (left side of screen)
- Has no major trunks in upper Abdomen below hepatic vein (contrast with Celiac and SMA of aorta)
- Portal Vein will be seen superficial to vena cava, but will not intersect
- Aorta sits immediately superficial to the Vertebrae
- Aorta bifurcation into iliac arteries occurs near Umbilicus
- Most critical site of Ultrasound is immediately superior to the Umbilicus (most common AAA site)
- Start in upper Abdomen at the epigastrium, and slide probe inferiorly
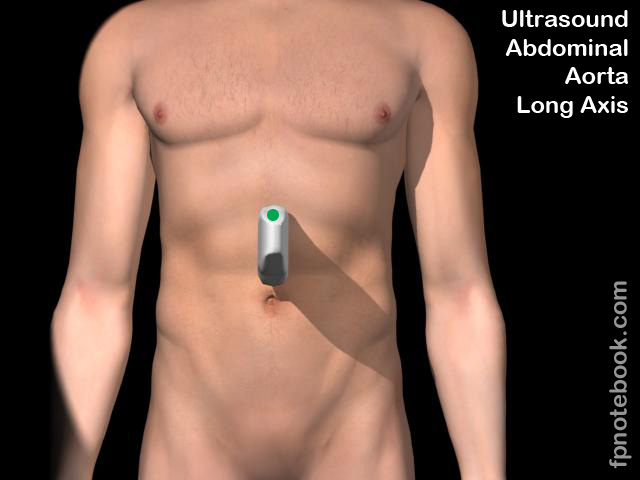
- Overview in long axis (other views are short axis)
- Consider starting with a long axis or longitudinal view (probe indicator to 12:00)
- Position probe in each of 2 locations
- Epigastrium
- Use liver as acoustic window and orient probe inferiorly
- Umbilicus
- View includes infrarenal aorta and bifurcation
- Epigastrium
- Differentiate aorta from the IVC at its right lateral side
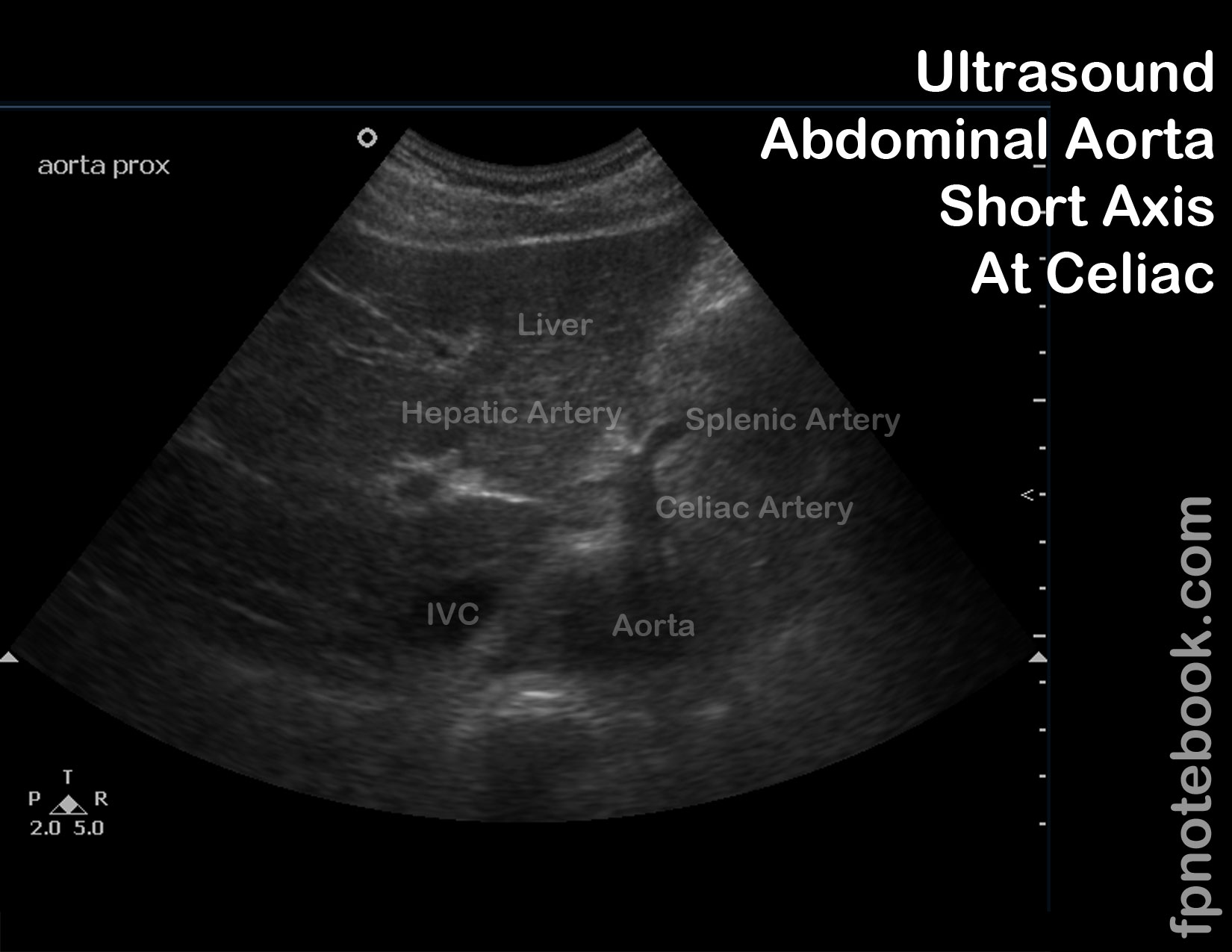
- Level of proximal aorta at Celiac Artery (short axis)
- Seagull appearance (immediately anterior to aorta)
- Celiac Artery forms the seagull's head
- Hepatic artery forms the wing on the patient's right
- Splenic artery forms the wing on the patient's left
- Seagull appearance (immediately anterior to aorta)
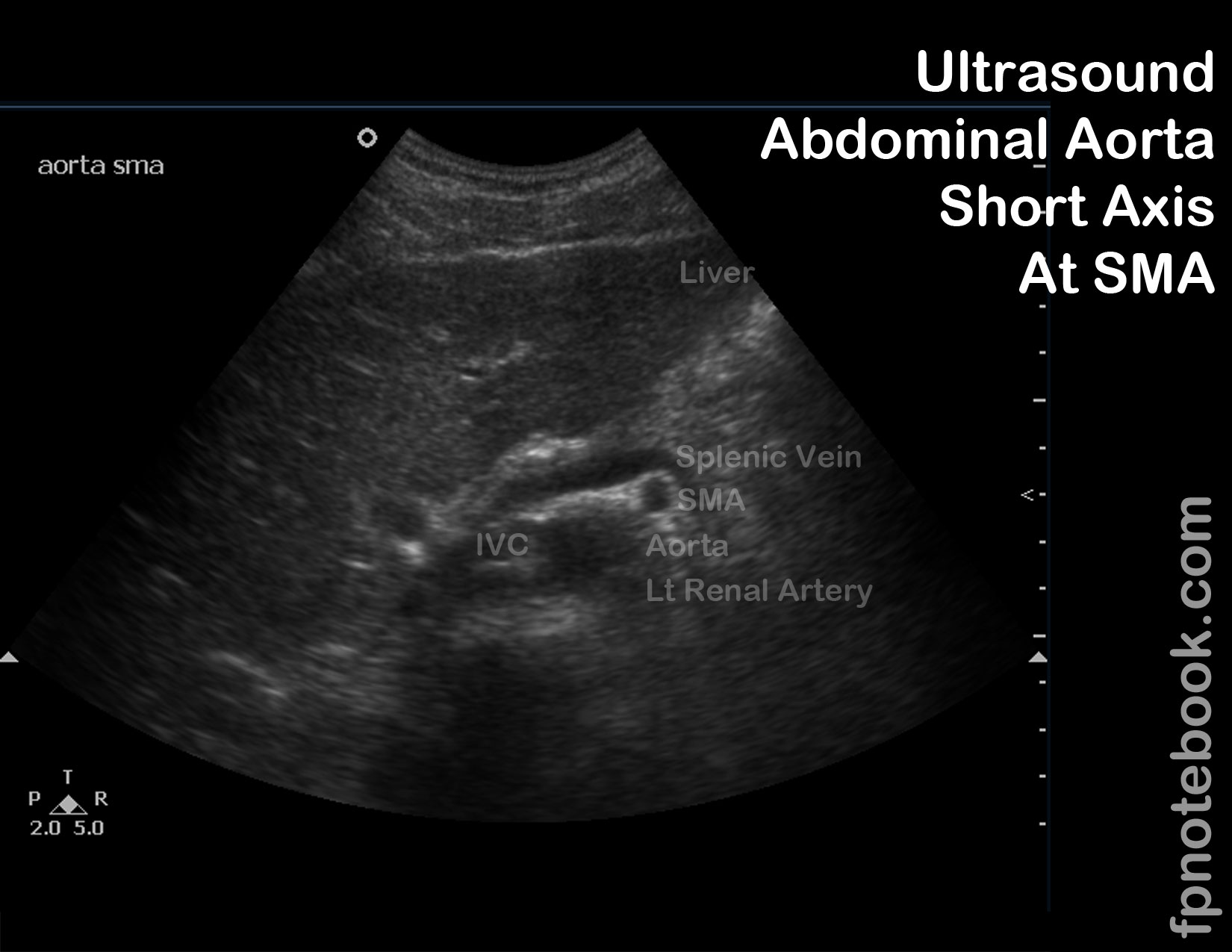
- Level of proximal aorta at superior Mesenteric Artery (short axis)
- Left renal vein crosses anterior to the aorta and posterior to the superior Mesenteric Artery
- Eyebrow over eye appearance
- Splenic vein forms the eyebrow
- Superior Mesenteric Artery forms the eye
- Level of proximal aorta at renal arteries (short axis)
- Difficult to visualize renal arteries at the aortic origin
- Level of mid-aorta, infrarenal, above bifurcation (short axis)
- No unique landmarks
- Most common site of AAA
- Level of distal-aorta at Umbilicus level or L4 (short axis)
- Aorta bifurcates into Iliac arteries
- Images
- Abdominal aorta anatomy
- Abdominal Aorta Long Axis
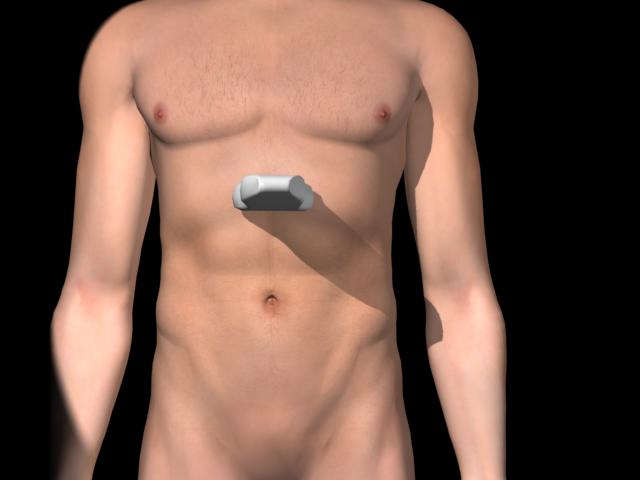
- Abdominal Aorta Short Axis - Proximal
- Abdominal Aorta Short Axis - Mid
- Abdominal Aorta Short Axis - Distal
- Abdominal aorta anatomy


- Imaging
- AAA Screening Protocol
- Obtain 3 short axis views (measuring from anterior aorta wall to posterior aorta wall)
- Proximal abdominal aorta (at Celiac Artery root)
- Mid abdominal aorta (at Mesenteric Artery root)
- Distal abdominal aorta (at iliac bifurcation)
- Obtain one longitudinal view (90 degrees from short axis view)
- Obtain at level to include distal aorta
- Technique
- Aorta Meaurements
- Measure aorta in short axis in AP diameter (anterior to posterior) from outer wall to outer wall
- Aorta diameter >3 cm is consistent with Abdominal Aortic Aneurysm
- Aorta diameter >5.5 cm meets criteria for elective repair
- Aorta diameter >7-8 cm is at high risk of rupture
- Pitfalls
- Aorta tapers as it descends towards the iliac arteries
- Aorta diameter >1.5x the normal diameter of the aortic segment is also considered aneurysmal
- Thrombus within aorta may be confused with aortic wall
- Thrombus typically forms anterior and lateral within the aorta
- Measure from anterior to posterior aorta walls (including the thrombus)
- Do not limit measurement to open lumen (underestimates aneurysm)
- Aorta tapers as it descends towards the iliac arteries
- Resources
- Abdominal Aortic Aneurysm Ultrasound Video (Dr. Perera, SonoSite)
- References
- Jorgensen (2012) Introduction and Advanced Emergency Medicine Ultrasound Conference, GulfCoast Ultrasound, St. Pete's Beach
- Noble (2011) Emergency and Critical CareUltrasound, Cambridge University Press, New York, p. 115-30
- Reardon (2016) Abdominal Aorta, Stabroom.com online video, accessed 4/1/2016
- Reardon (2011) Pocket Atlas Emergency Ultrasound, McGraw Hill, New York, p. 107-128
- Sparks (2002) Am Fam Physician 65(8):1565-70 [PubMed]