Gallbladder Ultrasound, RUQ Ultrasound
- See Also
- Efficacy
- Cholelithiasis
- Test Sensitivity for Gallstones: 95%
- Test Specificity high
- Can visualize Gallstones >= 2 mm
- Serial Ultrasound in 12-16 hours may demonstrate progression
- Increased gallbladder wall thickening
- Ultrasonic murphy's sign
- Evaluation
- Cholecystitis
- Findings suggestive of Cholecystitis
- Presence of Gallstones
- Thickened gallbladder wall
- Gallbladder distension
- Pericholecystic fluid
- Positive sonographic Murphy Sign (pain provoked when pressure applied directly to visualized gallbladder)
- Interpretation: Above findings present
- Cholecystitis Positive Predictive Value (PPV) 90%
- Interpretation: Above findings absent
- Cholecystitis unlikely
- Imaging
- Point of Care Ultrasound
- Positioning
- Patient starts supine
- May need to switch to left lateral decubitus or upright in difficult cases
- Images may improve (decrease rib shadowing) with a held deep inspiration
- Patients should not have eaten recently
- Gallbladder will contract after eating making visualization very difficult
- Patient starts supine
- Transducer
- Curvilinear transducer (large footprint abdominal probe, 2.5 to 5.0 MHz)
- Typical probe with best penetration and best visualizes common bile duct
- Phased-array probe (cardiac probe)
- Indicated if only view is lateral intercostal (due to overlying gas, patient position)
- See Right Intercostal Oblique Ultrasound View (part of FAST Exam)
- Curvilinear transducer (large footprint abdominal probe, 2.5 to 5.0 MHz)
- Precautions
- Scan gallbladder in both axes (short and long axis)
- Scan through a series of planes (serial cuts) in each axis
- Gallstones
- Scan gallbladder in both axes (short and long axis)
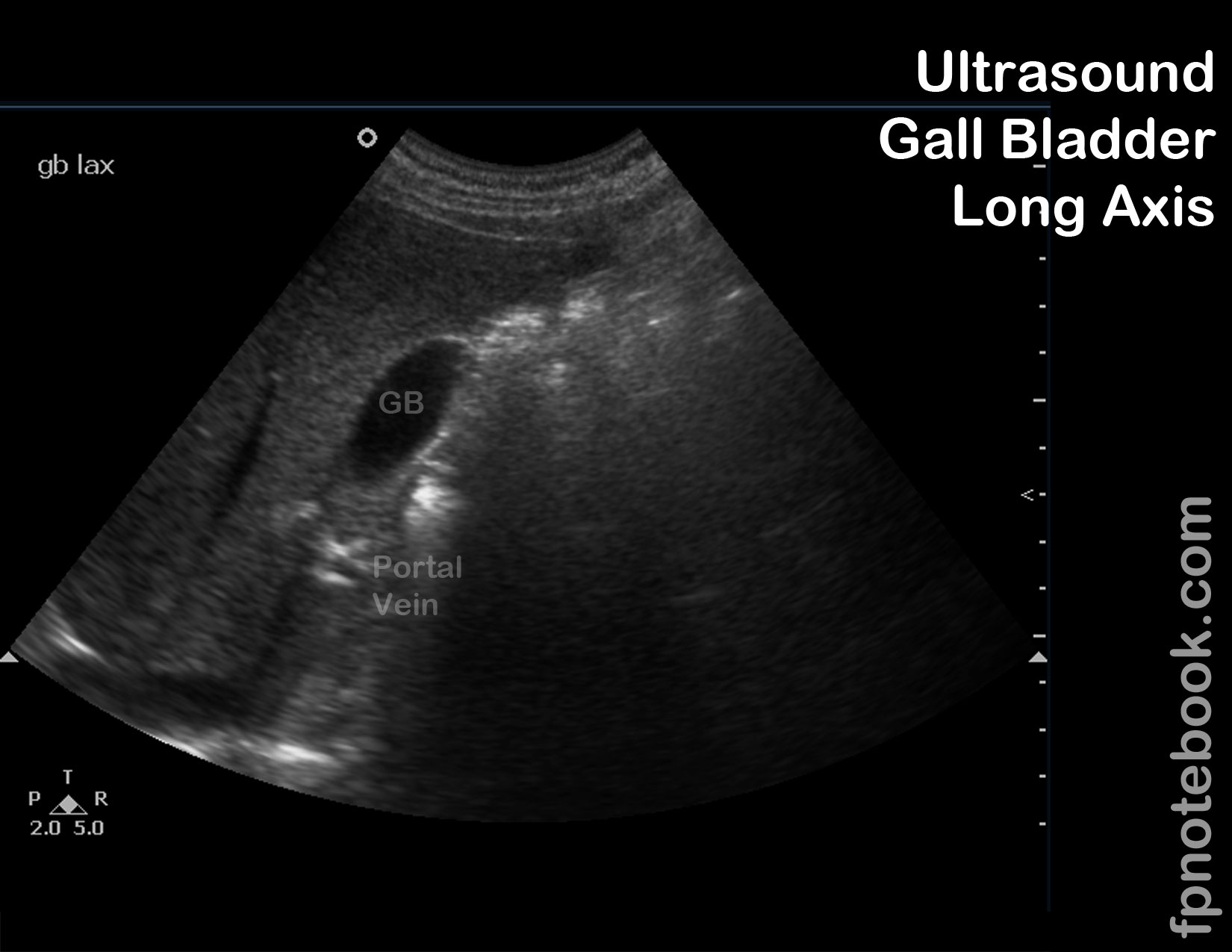
- Landmarks: Long Axis (longitudinal)
- Portal triad
- Appears as Mickey Mouse (Portal Vein as face, and CBD and HA as each of the ears)
- Anterior: Common bile duct (CBD) and hepatic artery (HA)
- Consider using color doppler (at low threshold) to distinguish hepatic artery and common bile duct
- Do not need to distinguish CBD from HA if both are small
- Posterior: Portal Vein
- Inferior Vena Cava lies deep to portal triad
- Gallbladder is medial to the portal triad
- Consider following the Portal Vein medially to identify the gallbladder
- Then rotate the probe obliquely to position the gallbladder in long axis
- Portal triad
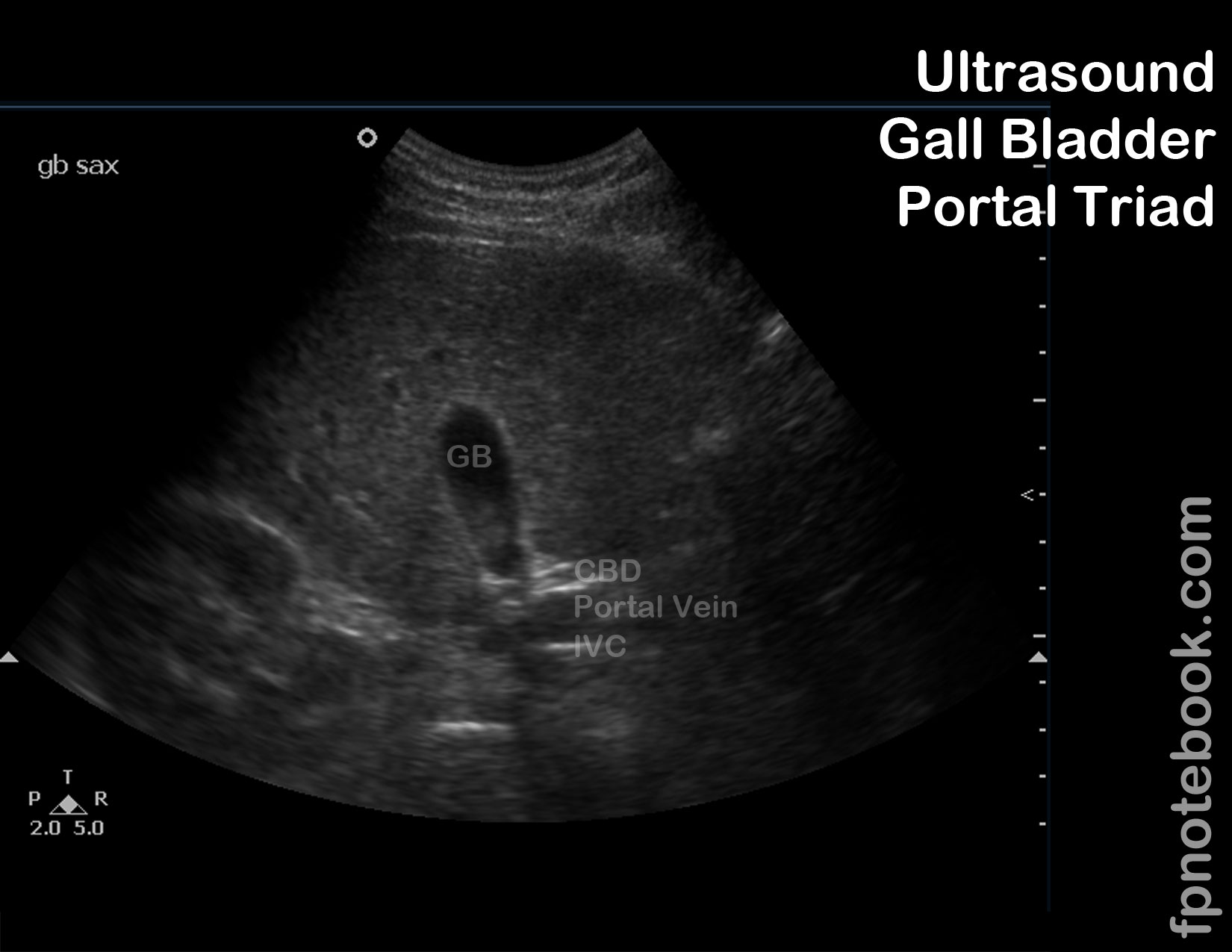
- Landmarks: Short Axis (transverse)
- Common bile duct (faint narrow line normally) in long axis
- Portal Vein (immediately below common bile duct) in long axis
- Inferior vena cava (~1 cm inferior to Portal Vein) in cross-section
- Images
- RUQ/GB Long Axis
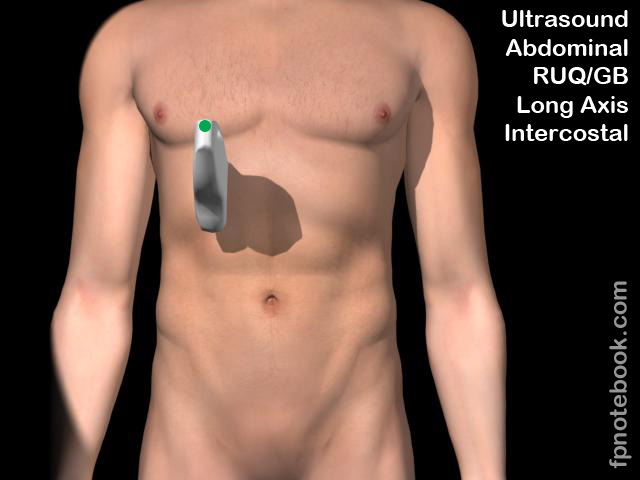
- RUQ/GB Long Axis - Intercostal
- RUQ/GB Short Axis
- RUQ/GB Long Axis
- Gallbladder localization
- Anterior Long axis or longitudinal approach
- Anterior Short axis or transverse approach
- Start with probe indicator at 9:00 with energy directed towards patient's right Shoulder
- Gradually tilt probe through an arch from head to foot
- Lateral Long axis or longitudinal approach
- Start at lateral oblique at Morrison's Pouch (as in FAST Exam)
- Slide probe anteriorly until Gall Bladder is visualized
- May require patient to take a deep breath to bring Gall Bladder below the level of rib shadowing
- Measurements
- Gallbladder anterior wall thickness
- Measure at crisp interface between liver and gallbladder, at mid-anterior wall (not at neck/fundus)
- Common Bile duct
- Measure in the bile duct's long axis where it lies above the Portal Vein
- Obstructed, dilated common bile duct will approach the size of the Portal Vein
- Gallbladder anterior wall thickness
-
Cholecystitis findings
- Common bile duct >8 mm diameter is considered dilated
- Borderline common bile duct diameter: 6-8 mm
- Post-op Cholecystectomy common bile duct diameter is normal up to 10 mm
- Gallbladder wall is thick (>3 mm) and echogenic
- Ultrasound Murphy's Sign (compression of gallbladder with probe increases pain)
- Pericholecystic fluid
- Common bile duct >8 mm diameter is considered dilated
-
Cholelithiasis (Gallstone) findings
- Gallstones are echogenic and when >3mm result in shadowing
- Gallstones are mobile and will move when patient changes position (contrast with immobile polyps)
- Gallstone in the gallbladder neck (especially if immobile) predicts impending Cholecystitis within ensuing days
- Normal findings
- Gallbladder sludge is a common finding when oral intake is decreased



- Resources
- Gallbladder Ultrasound Video (Part 1, Dr. Perera, SonoSite)
- Gallbladder Ultrasound Video (Part 2, Dr. Perera, SonoSite)
- Gallbladder Ultrasound Video (Part 3, Dr. Perera, SonoSite)
- References
- Mateer and Jorgensen (2012) Introduction and Advanced Emergency Medicine Ultrasound Conference, GulfCoast Ultrasound, St. Pete's Beach
- Noble (2011) Emergency and Critical CareUltrasound, Cambridge University Press, New York, p. 151-71
- Reardon (2016) Gallbladder Ultrasound, Stabroom.com online video, accessed 4/1/2016
- Reardon (2011) Pocket Atlas Emergency Ultrasound, McGraw Hill, New York, p. 129-61
- Reardon (2013) Emergency Ultrasound Course, 3rd Rock Ultrasound, Minneapolis, MN